
Translate this page into:
Significance of the Development of a Cardiovascular Disease Surveillance and Reporting System in India
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Cardiovascular disease (CVD) is the single largest cause of global morbidity and mortality and is the leading cause of death in the Indian subcontinent projected to contribute to deaths expected to double by 2015. The social and economic impact of these staggering projections highlight the need for a centralized effort to monitor and evaluate behavioral and physiological risk factors for CVD. Limited evidence on existing surveillance systems suggest that the key to an effective monitoring and evaluation (M and E) program for CVD surveillance in India relies upon the World Health Organization's STEP-wise model. Key recommendations for the Ministry of Health include the development of a national CVD surveillance program with expertise and a quality-improvement mechanism to receive continuous input from similar surveillance programs in likeminded countries. Structure of the surveillance system would include; (1) the development of process measures for CVD risk factor’ based surveillance M and E systems for early detection of CVD at the local-level, (2) the development of trigger based data reporting responsibilities to State-based monitoring teams including incentives for accuracy in data reporting and the use of data-driven evidence to target risk specific intervention and prevention on Central Government monitoring teams with reporting feedback to the State and local-levels and (3) the creation of health policy to require the use of data to target risk specific prevention for intervention and developing local technical capacity. Such a system would provide significant cost and social benefits, presenting an evidence based data driven cost-effective business case for scale-up and potential use in areas comprising similar demographics. Future research should focus on the inclusion of a systematic critique of the reported data for the challenges to surveillance systems in India and the examination of the effect of an incentivized reporting system on the states. Further inquiry into the types of reporting and lessons from other countries’ surveillance programs with alternative strategies to a national approach should address potential imitations at the ground or peripheral levels.
Keywords
Cardiovascular disease
Chronic disease model
Data collection
Disease reporting
India
Risk factor surveillance
World Health Organization STEPwise approach

CHRONIC DISEASE BURDEN IN INDIA
India is a key global player, with the world's second largest population and projected economic growth.[1] However, its contribution to the overall global burden of disease is high and although projected to worsen by 2025,[2] considerable effort is being placed on the prioritization of resources to strategize next steps and combat this trend. As a result, efforts to constantly re-prioritize disease control strategies within India, coupled with an increased ability to synthesize evidence based practices and conduct surveillance with greater accuracy are all necessary. Particularly in the case of chronic diseases such as cardiovascular disease (CVD), the burden is increasing Figures [1 and 2]; it is not only one of the leading causes of death, projected to contribute to the rising mortality in India;[3] [Figure 3] with deaths due to CVD expected to double by 2015[4],[5] and projected to be the largest cause of death and disability in India by 2020 [Figure 4]. According to a paper published in the lancet,[6]"responding to the threat of chronic diseases in India," the estimated prevalence of coronary heart disease is 3-4% in rural areas and 8-10% in urban areas among adults older than 20 years, representing a two-fold rise in rural areas and a six-fold rise in urban areas over the past four decades. A total of 30 million people are estimated to have coronary heart disease in India in 2003; 14 million in urban areas and 16 million in rural areas,[7] affecting the productivity of the workforce and the economic output of the country.[8] Improved surveillance techniques are required to allow for precision to assess the impact of the epidemic in the country. The purpose of this paper is to briefly review the existing limited literature on the history of disease reporting in India, and to propose the case for the development of a national surveillance system for CVD within India. The need for an effective measure of incidence, prevalence as well as monitoring and evaluation (M and E) of CVD in targeted areas within the country is required in order to introduce standards for reporting, and to ultimately improve reliability and validity of control measures within India.
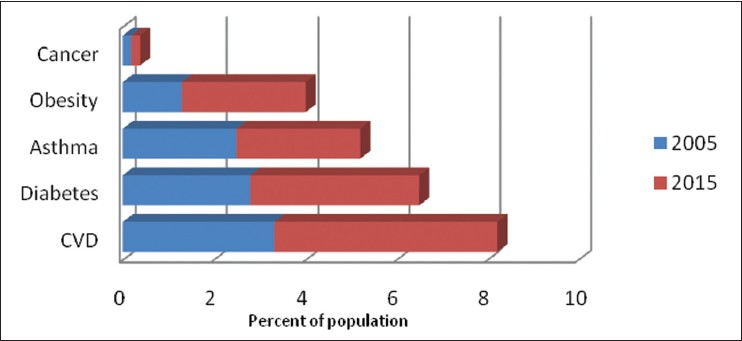
- Prevalence of chronic diseases in India: By disease (y axis) and percent of population (x axis)
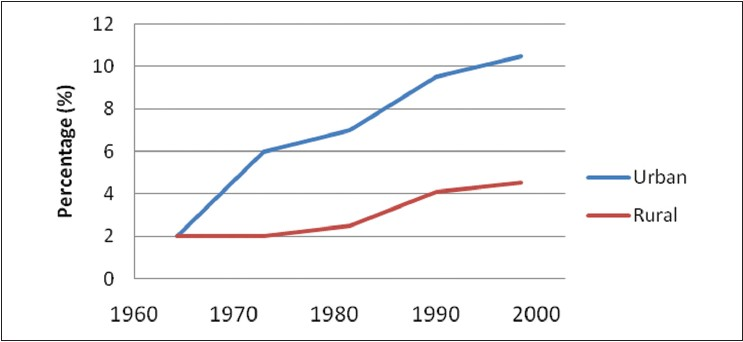
- Prevalence of cardiovascular disease in India: By percent of population (y axis) and year (x axis)

- Deaths due to cardiovascular disease in India: By population in millions (y axis) and year (x axis)
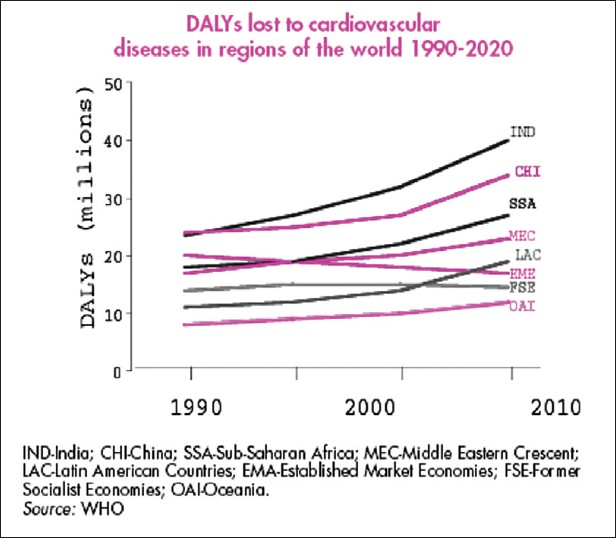
- Disability adjusted life years lost due to cardiovascular disease: By population in millions (y axis) and year (x axis)
SIGNIFICANCE OF DISEASE REPORTING IN INDIA
Disease reporting in India has always been a challenge - the central government in New Delhi does not keep centralized statistics regarding the epidemiology of diseases since such records are the responsibilities of the state. In addition, communication gaps between the states and the central government isolates states to fend for their own health concerns and are often reported.[9]
Problems are magnified in the case of chronic diseases since they have been largely ignored due to the central government's sole focus on communicable diseases such as malaria, tuberculosis and human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) where most immediate attention and resources have been used to act, respond, diagnose, treat and reduce the transmission and incidence of the disease. Although the comprehensive national database of CVD studies contain associated epidemiology and prevention studies in India from the recent past, it is static and remains outdated since 2002. Even though this guide serves effectively as a reference tool for the advocacy of future policy and research, it is clear that ongoing surveillance of chronic diseases in India is extremely important in order to provide an accurate estimate of disease prevalence and incidence and ultimately assist efforts to reduce the non-communicable disease burden in the country.
HISTORY OF DISEASE REPORTING
Ever since the 1945 cholera epidemic resulted in significant morbidity and mortality causing huge losses to the economy[10] the focus on surveillance systems has emphasized the preparation for the potential spread of disease outbreaks.
Existing surveillance systems for disease reporting in India have operated; the centralized system also referred to as the National Surveillance Program for Communicable Diseases (NSPCD)”[11] has operated since 1997 under the National Institute of Communicable Diseases (NICD). NICD has served as the national coordinating agency in the central government, operating as part of the Director-General of Health Services under the Government of India. The centralized system has focused on strengthening the state, district and taluka levels in the identification of the epidemiology of communicable diseases allowing for an effective, unified and coordinated response. Such surveillance and disease reporting has been intended to provide a clear interconnected strategy to operate in 101 districts of 35 states and 2 union territories. The NSPCD has also been responsible for the development of rapid response team (RRT) guidelines, laboratory and computer manuals and training materials, in addition to providing the training of state RRTs, strengthening the network and sharing of information amongst the National and Regional laboratories, the establishment of rapid communication networks, institution of technical review committees and the overall co-ordination, M and E of the epidemic under surveillance.
Disease reporting in India took a new turn for infectious diseases, particularly with the onslaught of the HIV/AIDS epidemic in the early to mid-1990’s; the increase in reported cases over the course of the epidemic for the past two decades and the spread took a toll on the productivity of the Indian workforce and the economic output of the country.[8] In addition, associated disability adjusted life years (DALY’s) due to HIV/AIDS resulting from this inability to diagnose and treat effectively was devastating.[12] For this purpose, AIDS specific surveillance systems were created under the auspices of the National AIDS Control Organization (NACO):[13] Under the purview of the Ministry of Health and Family Welfare, the Government of India's NACO branch served as one of the identified organizations chartered to coordinate the response to the HIV/AIDS outbreak to conduct disease surveillance. The program launched in 1992 was a response to the increasing number of HIV/AIDS cases within India. Under this program, the annual structured sentinel surveillance was conducted wherein essential information on the dynamics and trends of HIV seroprevalence was collected throughout the country. In addition to carrying out cross sectional surveillance studies at regular intervals throughout the year in community based settings, NACO also conducted surveillance at specific clinics and health facilities that served high-risk populations, a strategy that has been proven to be more cost effective than the general community surveillance. Surveillance using the latter strategy is targeted at antenatal clinics, sexually transmitted disease clinics, rural sites, migrant population sites, truck driver stops and other high-risk clinic sites. Each laboratory testing site reports to a two or three member state team comprised of an epidemiologist and a microbiologist from local medical colleges. These teams in turn report to six regional institutions throughout the country which directly report to the coordinating body of the central government.
On the other hand, the decentralized system of state based reporting commonly referred to as the “Integrated Disease Surveillance Project (IDSP)”[14] reporting system initiated in 2004 was designed to improve the overall efficiency of disease surveillance within India by its use in health planning, management and evaluating control strategies. Initially funded by the World Bank, the state based system of reporting includes the transmission of information regarding associated risk factors or symptoms of communicable diseases to include a wide range of target infectious diseases, such as Malaria and HIV/AIDS. The intention of the state based approach to reporting is to detect early warning signals of impending outbreaks and help assist in the initiation of an effective response in a timely manner. Major components of this type of reporting strategy are focused at the integration within the state based organizational levels and decentralization of surveillance activities, as well as includes a plan to strengthen public health laboratories for testing.
LIMITATIONS TO EXISTING DISEASE REPORTING APPROACHES
The challenge with these approaches to disease reporting have been numerous; firstly, such reporting have been too vertical for a large country like India, in addition to the fact that centralized level responses to disease outbreaks can also result in huge delays in responding to outbreaks that especially require immediate attention. In addition, the approach has been retroactive in nature, allowing for the retrospective reporting of data after the outbreak has occurred.
Secondly, a lack of accuracy in the data generated by this approach is commonplace; with the complex hierarchy of people involved in the process of data collection and analyses and the different levels in the approach as well as the limited number of those individuals or organizations having access to the reported data result in a general sense of lack in accountability and inaccuracies in the data being collected. Such inaccuracies in data lead to a skewed perception and misrepresentation of the problem.
Thirdly, it is obvious that such data has tremendous limitations. Such disease reporting surveillance systems have merely resulted in monthly reporting from mostly bureaucratic government agencies on a set of diseases, without reference to the private and non-formal sector and as a result the data is misrepresented; mainly being numbers without having much meaning. More importantly, such data has not been used for action in the local community. In addition, at the district levels, there is no single person whose primary responsibility is to survey diseases. Health officers’ have multiple responsibilities and are therefore not expected to do full time surveillance, but they are usually in charge. As a result, the understanding that the data can only be “as good as it can be” has contributed to the inaccuracy in the data management resulting in dishonest data.[15]
MODELS OF CHRONIC DISEASE SURVEILLANCE FOR CVD
The contributing factors for the growing burden of CVD are the increasing prevalence of cardiovascular risk factors especially hypertension, dyslipidemia, diabetes, overweight or obesity, physical inactivity and tobacco use.[6] It is an area where major health gains can be made through the implementation of models of chronic disease surveillance where primary care interventions and basic public health measures target diet, life-styles and the environment.
Attempts at the use of such CVD risk factor surveillance systems have been effective; as part of collaboration between the Centers for Disease Control and Prevention (CDC) and the Russian National Center, for Preventive Medicine, a telephone-based behavioral risk factor surveillance survey was developed and tested in Moscow[16] Although such surveillance used a telephone based system to collect data in Russia's deteriorating infrastructure, the surveillance system was proven to be an effective means of risk factor control for CVD. Another similar study conducted amongst an industrial population in Chennai, India[17] also emphasized that the treatment and control of diabetes and hypertension as risk factors of CVD were better controlled in the population under risk factor surveillance than that in the general population. Other studies have replicated these findings in Iran[18] as well has been recommended by the US Center for Disease Control in their action plan on the heart disease and stroke prevention national initiative.[19] As a result, evidence suggests that the key to an effective program for non-communicable disease relies upon the M and E of behavioral and physiological risk factors.
WHO STEPWISE MODEL FOR CVD SURVEILLANCE
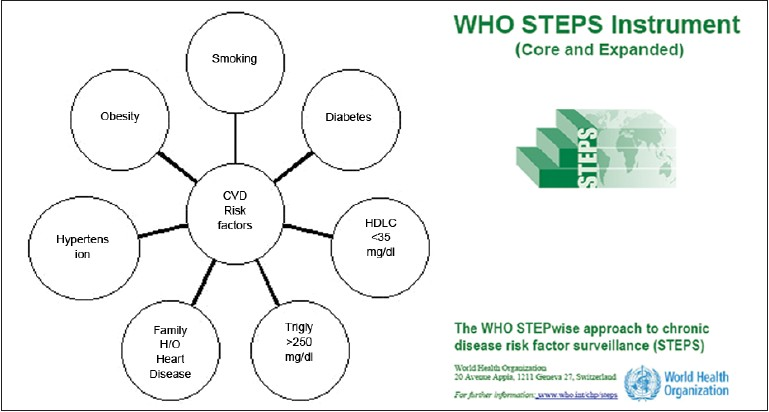
The WHO's stepwise model to chronic disease risk factor surveillance presents a theoretical framework for approaching the use of such behavioral and physiological risk factors surveillance systems in the country [Chart 1]. The model uses behavioral measurements such as tobacco use, alcohol consumption and diet; physical activity and lifestyle modification and other biological testing measurements as markers for CVD risk and provides surveillance information useful for early targeting of those populations at high risk, as well as presenting opportunity on potential interventions [Chart 2]. The use of this model for surveillance of stroke risk factors and mortality in India has already been successful.[20] Such surveillance clearly has the potential to present vital National Health Metric data required for effective public policy and in the allocation of prioritized resources for prevention and presents an opportunity for the Indian Government for integration into existing disease reporting infrastructure.
- Cardiovascular disease behavioral and physiological risk factors
CHALLENGES TO SURVEILLANCE IN INDIA
Surveillance needs at various levels; State, Taluka, District, may serve different purposes, but all components of the system should be designed to best inform the strategies for preventing CVD that are best implemented at that level.[21] Surveillance data are also critically important at both the state and local level to develop, implement and evaluate any program on CVD prevention and control. This is more important in the Indian subcontinent as “health” is more of a state subject than it is in the Indian central government. State and local public health agencies require relevant surveillance data, specific to their state or local area, to use in developing and seeking funding for targeted intervention programs, informing policy makers and guiding policy decisions and planning and evaluating programs. Data as such are needed to inform state and local decision makers about the impact of current and future policies pertaining to nutrition and physical education programs in schools, universities and work place environments, tobacco taxes and other control policies and, as well as other prevention programs. Because funding for CVD prevention programs is low relative to the public health burden of these diseases in most states and local areas, public health agencies must carefully prioritize their preventive efforts and continually evaluate ongoing programs to assess and improve their impact. State or local populations at particularly high risk for CVD can be identified and targeted for intensive interventions that may not be feasible or efficient on a broader scale. State and local public health agencies cannot design, implement and evaluate such programs without relevant, reliable, accurate and timely surveillance data.
RECCOMENDATIONS FOR THE MINISTRY OF HEALTH
Key recommendations for the Ministry of Health include the development of a national CVD surveillance program with expertise and a quality-improvement mechanism to receive continuous input from similar surveillance programs in likeminded countries. Structure of the surveillance system would include (1) the development of process measures for CVD risk factor’ based surveillance M and E systems for early detection of CVD at the local-level, (2) the development of trigger based data reporting responsibilities to State-based monitoring teams including incentives for accuracy in data reporting and the use of data-driven evidence to target risk specific intervention and prevention on Central Government monitoring teams with reporting feedback to the State and local-levels and (3) the creation of health policy to require the use of data to target risk specific prevention for intervention and developing local technical capacity.
PROCESS MEASURES
Risk factor based surveillance M and E systems for early detection of CVD at the local-level should include the monitoring of risk factors - behavioral and physiological as described in the WHO STEPS model as seen in Chart 2. The model should be tailored to India by the definition of the core risk factors and the development of guidelines to accompany the core measures. Mortality and morbidity attributed to the core risks should be reported as overall rates by hospitals and community based organizations as seen in the proposed structure reporting for CVD surveillance as in Chart 3.
- WHO STEPS Instrument for cardiovascular disease risk factor surveillance

- Proposed reporting structure for cardiovascular disease surveillance
INCENTIVIZED REPORTING
Economic benefits for accuracy should be embedded into the development of trigger based data reporting responsibilities to state-based monitoring teams including data reporting and the use of data-driven evidence to target risk specific intervention and prevention on Central Government monitoring teams with reporting feedback to the state and local-levels. An autonomous and non-partisan entity should serve as a Reporting Taskforce, which would include the buy-in and collaboration of key stakeholders and public-private partnerships. Such incentives for compliance with a proposed incentivized reporting framework seek to address limitations at the ground level or peripheral level. Recommendations for incentivized reporting are summarized in the proposed incentivized reporting framework as seen in Chart 4.

- Proposed incentivized reporting framework
HEALTH POLICY AND NEED FOR DEVELOPING LOCAL TECHNICAL CAPACITY
Health policy should be created requiring the use of data to target risk specific prevention, requiring an evidence based rationale for intervention. Such policies would eventually help develop an evidenced based prevention policy which will seek to drive behavior change and resources for added value and capacity in the workforce.
CHANGING FACE OF INDIA
Numerous organizations in India comprise a range of infrastructures. Standardized surveillance would need to be embedded into the changing information systems of the country such as the Citizens Smart Card Bill (2006) with financial pledges made for data reporting. Developing local capacity and allocation of additional resources diffused through to the state based levels for carrying out such standardized surveillance will inevitably present numerous challenges however. For a surveillance system to function effectively in India, one of the first requirements would be to recruit a large number of reporting units such as clinics, hospitals, academic medical centers, private hospitals practitioners and all practitioners would need to meet certain standard requirements such as basic computer skills. These individuals would then need to be imparted with education and basic training through meetings and visits by public health professionals on the importance of reporting and/or risk factors of importance. An officer at the district level would then coordinate the collection of data and analysis for their zonal distribution. Creating an autonomous non-partisan body for CVD disease surveillance with committed professionals manning a nationwide network of units can have a beneficial effect on the disease control and epidemic responsiveness of India. This will only be possible if professionals are appointed from outside the state system, with the time to do data collection and analysis. Such individuals would also serve to act as a bridge with the private sector in addition to being allowed to act as an independent entity within the system. Although answerable to a national level surveillance body, possibly an agency appointed by the Ministry of Health, with little or under no pressure to either under-report or over-report. The effects of such a new reporting structure would have to be continuously studied and monitored starting with one state as well as the range of perception amongst India's consumers – the patients.
FUTURE STEPS
Evidence on existing surveillance systems clearly suggest that the key to an effective program for non-communicable disease relies upon the M and E of behavioral and physiological risk factors. The WHO's STEP-wise model to chronic disease risk factor surveillance clearly presents an opportunity for the Indian Government to integrate such surveillance systems into the disease reporting infrastructure of the country. Health Metric data will provide mounting evidence required for effective public policy and for the allocation of prioritized resources for prevention. Although, developing local capacity and allocation of additional resources diffused through to the state based levels for carrying out such standardized surveillance present numerous challenges, it is still achievable and tackling this with the creation of a national surveillance system for CVD is on the road to the future of improving the burden of chronic diseases in India. Future research should focus on the inclusion of a systematic critique of the reported data for the challenges to surveillance systems in India and the examination of the effect of an incentivized reporting system in one state. Such an examination should focus on understanding the impact of an incentivized reporting system on accuracy in data versus a non-incentivized approach. Further inquiry into the types of reporting based on social context should address whether reporting should be anonymous or name based as well as incorporate the regional heterogeneity and high risk groups. Lessons from other countries’ surveillance programs and alternative strategies to a national approach should also address potential imitations at the ground or peripheral levels.
ACKNOWLEDGMENTS
The author would like to thank Dr. James Seward, Clinical Professor of Medicine and Global Health Sciences Faculty at the University of California, San Francisco for mentorship and Dr. John Ziegler, Professor Emerita and Ex-Officio Director of Global Health Sciences at University of California, San Francisco and two anonymous reviewers for useful comments during the review of the paper.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- www.scribd.com [Internet]. c2008-01. 2009. Health care in India: Report Highlights. United Sates: Boston Analytics, Inc.; Available from: http://www.scribd.com/doc/88298150/Healthcare-Analysis-Boston-Report
- [Google Scholar]
- Health care in India - 2025: Issues and prospects India Planning Commission [Internet]. Available from: http://planningcommission.nic.in/reports/sereport/ser/vision2025/health.pdf
- Emerging epidemic of cardiovascular disease in developing countries. Circulation. 1998;97:596-601.
- [Google Scholar]
- Impact of HIV/AIDS on the national economy of India. Health Policy. 1999;47:195-205.
- [Google Scholar]
- Disease Surveillance in India: Framework for Implementation of revised IHR 2005 in India. [Internet]. Available from: http://www.queensu.ca/iigr/Res/phf/06-2/06-2agenda/IND.ppt
- World Health Organization [Internet]. Geneva, Switzerland: Global Taskforce on Cholera Control; Available from: http://www.who.int/cholera/technical/prevention/control/en/index1.html
- www.hetv.org [Internet]. India: Health Education to Villages. National Surveillance Programme for Communicable Diseases (NSPCD). Available from: http://hetv.org/india/mh/healthstatus/communicable-diseases.htm
- [Google Scholar]
- Chapter 18: HIV/AIDS Prevention and Treatment. In: Jamison DT, Breman JG, Measham AR, eds. Disease Control Priorities in Developing Countries (2nd ed). Washington (DC): World Bank; 2006.
- [Google Scholar]
- National AIDS Control Organisation, Ministry of Health and Family Welfare, Government of India. C2006-2007. UNGASS Country Progress Report 2008 India. Available from: http://data.unaids.org/pub/report/2008/india_2008_country_progress_report_en.pdf
- [Google Scholar]
- Government of India, Ministry of Health and Family Welfare. Intergrated Disease Surveillance Project. Available from: http://idsp.nic.in
- [Google Scholar]
- Disease surveillance vital to control epidemics, The Hindu. Available from: http://www.thehindu.com/thehindu/op/2005/12/11/stories/2005121100041400.htm
- Monitoring behavioral risk factors for cardiovascular disease in Russia. Am J Public Health. 2001;91:1613-4.
- [Google Scholar]
- Surveillance for risk factors of cardiovascular disease amongst an industrial population in southern India. Natl Med J India. 2008;21:8-13.
- [Google Scholar]
- An Overview of a National Surveillance Program in Iran for Prevention of Chronic Non-communicable Diseases from Childhood: CASPIAN Study? 2009. Iran J Public Health. 38:102-6. Available from: http://journals.tums.ac.ir/abs.aspx?org_id=59&culture_var=en&journal_id=5&issue_id=1545&manuscript_id=13371&segment=en
- [Google Scholar]
- CDC Action Plan, Heart Disease and Stroke Prevention: Time for Action. :13-32.
- WHO - India. Available from: http://www.searo.who.int/india/topics/cardiovascular_diseases/NCD_risk_CVD_surveillance_for_industrial_settings.pdf
- Cardiovascular Disease (CVD) surveillance and health promotion in Industrial settings, not a formal publication of the World Health Organization (WHO); is a product of the APW SE/06/226543 between IC Health and WHO and submitted to WHO on 10 August, 2007




