
Translate this page into:
The Effect of Aromatherapy with the Essential Oil of Orange on Pain and Vital Signs of Patients with Fractured Limbs Admitted to the Emergency Ward: A Randomized Clinical Trial
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background and Objective:
Pain is an emotional and unpleasant experience associated with actual or potential tissue damage. The literature shows no study on the effect of aromatherapy with the essential oil of orange on unpleasant feelings of patients with fractured limbs. In this regard, this paper aims at studying the effect of aromatherapy with the essential oil of orange on patients with fractured limbs admitted to the emergency ward.
Methods:
Sixty patients admitted to the emergency ward of Vali-e-Asr Hospital were selected by purposive sampling method and then were divided into two groups of control and experiment by block method. This study was done in one shift work (morning or afternoon). Four drops of the orange oil were poured on a pad and were pinned with a plastic pin to the patient's collar, about 20 cm distant from head. The old pad was replaced by the new one every 1 h. The patients' pain and vital signs were checked every 1 h for at last 6 h. The data were analyzed by SPSS Version 21.
Results:
Forty (66.7%) patients were male and twenty (33.3%) were female. Their age average was 37.93 ± 18.19 years old. The most fractured cases were in the scapular (11 patients [18.3%]). Friedman test showed that pain in the experiment group (P = 0.0001) decreased significantly rather than the control group (0.339). However, in vital signs, there could be found that no significant change between the two groups was seen.
Conclusion:
Aromatherapy with orange oil can relieve pain in patients with fractured limbs but has no effect on their vital signs. Therefore, aromatherapy with orange oil can be used as a complementary medicine in these patients.
Keywords
Aromatherapy
emergency ward
limb fracture
orange oil
pain
vital sign

INTRODUCTION
According to the definition by International Association for the Study of Pain, pain is an unpleasant sensory and emotional experience.[12] Pain relief by reducing transferring painful data to the central nervous system and optimizing analgesia treatment can reduce mortality and morbidity in patients.[345] Lack of pain control can activate the sympathetic nervous system and increase morbidity and mortality in patients. Indeed, the sympathetic system activities can increase myocardial oxygen consumption and lead to, in some cases, ischemia and even myocardial infarction (by decreasing oxygen due to coronary artery contraction and inhibition of local vasodilator mechanisms).[3456] Another important side effect of stimulation of the sympathetic nervous system is reducing the gastrointestinal motility delay in stimulation of the digestive system (ileus).[34567] Lack of proper pain management in patients consequences impaired respiratory dysfunction in patients, especially during pain in abdomen and thoracic regions.[7] Moreover, pain has psychological effects as well and is regarded as the main reason for fear, anxiety, distress, and disappointment.[8] There are different ways to control pain including systemic analgesics (narcotics and nonnarcotics) and local anesthesia techniques; each can be prescribed according to the patient's medical condition.[9] A safe way that can control the pain with no side effects such as respiratory problems, pruritus, or hemodynamic dysfunction is ideal.[10]
Fractures and orthopedic surgery cause severe pain in patients and applying narcotic analgesics is necessary to use narcotic analgesics.[111213141516] Since the narcotic analgesics have general side effects such as respiratory problems, sedation, nausea and vomiting, symptoms of tolerance or withdrawal syndrome in patients, using nonpharmacological methods as complement rather than alternative interventions are recommended. In this regard, there are methods in complementary medicine by which nurses can help patients.[1718] They need to be prescribed by a physician or, in some cases, nurses avoid prescribing them, due to fear of side effects or make longer the time between doses. In this regard, using pharmacological drugs with nonpharmacological methods can be helpful and more efficient than methods.[19] Aromatherapy is the controlled use of natural aromatic oils to enhance psychological and physical well-being and is used as a part of nursing in many countries including Switzerland, Germany, England, Canada, and America.[20] The aromatic oils are extracted from aromatic plants, which are anti-inflammatory, antimicrobial, and reduce pain and stress.[20212223] In fact, applying aromatherapy is common, and it is the second complementary method among nurses since its clinical applications.[24] It has been proved that inhalation of the essential oil of orange can reduce the labor pain.[25] It also can stimulate the central nervous system, enhance moods, cause sedation and relief. It is an antispasmodic, an anti inflammatory, an antibloating, a food digestive, and a diuretic, and can lower the blood pressure. Its active substances are limonene and Flanders Citral (Levomenthol).[2627] Massage and aromatherapy with a combination of ginger and orange oils were effective in relieving knee pain in the 1st week among patients with osteoarthritis.[28] A study has shown that edible oil of orange can reduce breast pain caused by premenstrual syndrome.[29]
Considering the importance of pain and proper management of pain in patients and few researches on the relationship between aromatherapy and pains of fractured bones, this paper aims at studying the effect of aromatherapy with the essential oil of orange on pain and vital signs of patients with fractured limbs admitted to the emergency ward.
METHODS
This research is a clinical trial registered in the Center of Clinical Trial in Iran under code IRCT201607124519N6. Samples size was obtained by the following formula.[30]

According to the comparison of means formula and reference 30, the sample size for each group was estimated as 30. In the emergency ward of Vali-e-Asr Hospital, sixty patients were selected by the purposive sampling method and were divided into two thirty-patients groups of experiment and control by blocking method. The collecting data tools were a demographic questionnaire and self-report pain scale measured by the 10-item visual analog scale (VAS). The vital signs were checked by the researcher of that shift. This research was done in one shift work (morning or afternoon). The patients were fractured limbs admitted to the emergency ward of Vali-e-Asr Hospital in Arak, who must undergo orthopedic surgery voluntarily participated in this trial (they were matched based on their age, sex, type of fracture, and the initial pain). As patient entered to the emergency ward, for intervention, four drops of the essential oil were poured on the pad and were pinned with a plastic safe pin to the patients' collars with about 20 cm distant from the head and the pads were replaced with new ones every 1 h. The pain and vital signs in patients were checked every 1 h for at last 6 h. Since aromatherapy was used as a complementary medicine, the common standard treatments of pain in the ward have been performed to test and control groups.
Inclusion criteria
Patients with over 18 years old, no history of chronic pain, vision disorders, respiratory problems, and with mental and smell health, could participate in this research could participate this research. The informed consents were obtained from the participants.
Exclusion criteria
Patients with lack of interest in participating or withdrawing while performing the research and having any allergic symptoms while performing the research were excluded from the study.
Collecting data tools
The VAS (0–10) was used to evaluate the pain. This scale is graded between 0 and 10; 0 shows no pain and 10 implies the most severe pain. The patients show their pain by pointing on the right scale. This scale allows the patients to show their pain freely.[31] This scale is the most widely used pain evaluation tool in the world.[31323334] In addition to validity and reliability, this tool is easy to use. Zero, in this scale, shows no pain, 1–3 shows mild pain, 4–6 moderate, 7–9 severe, and 10 indicates very severe pain.[32] Many studies out of Iran have proved its validity and reliability.[33] In Iran, the reliability of this scale was confirmed with correlational coefficient 0.88[34] [Figure 1].

- The Visual Analogue Score, VAS (0-10)
Ethical considerations
This project has been registered under code IR. ARAKMU. REC.1395.111. The personal characteristics of all subjects of the research have been kept confidential. All participated voluntarily, and the informed consents were obtained. The subjects could withdraw whenever they wanted.
RESULTS
Sixty patients participated in this research, 30 in the intervention and 30 in the control group [Diagram 1]. Forty (66.7%) patients were male and 20 (33.3%) were female. Their age average was 31.93 ± 18.19 years old; the youngest was 18 and the oldest patient was 72 years old. Thirty-seven patients (61.7%) were married and 23 (38.3%) were single. Eleven patients (18.3%) had diploma, 8 (13.4%) had academic studies, and 41 patients (68.3%) had lower grades. The subjects in the two groups have the same demographic information, and there could be found no significant differences.

- Flow Diagram of Enrollment
Fisher's exact test results showed that the distribution of fractures in the two groups has no significant difference. Although the most common fractures were of the scapula with 11 patients (18.3%) [Table 1].

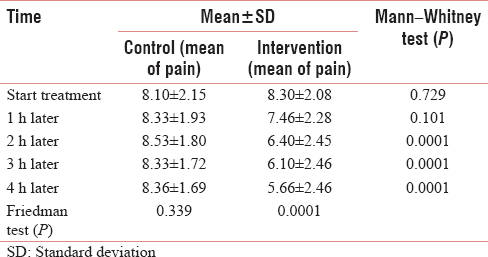
The results showed no statistically significant difference in mean pain scores in different times. However, pain scores in the intervention group have significant differences at different times (P = 0.0001) and with increasing duration of pain was significantly reduced [Table 2].
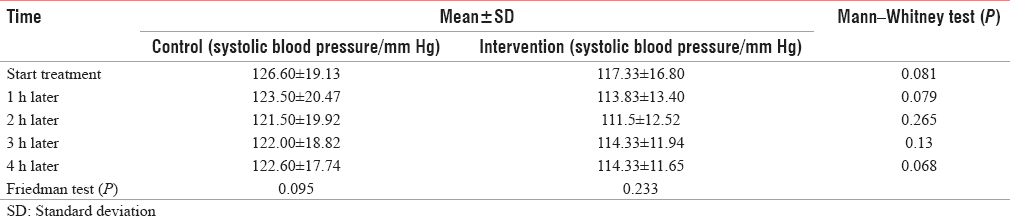
The results showed, at all times, no statistically significant difference in mean of systolic blood pressure. This means that changes in systolic blood pressure in both groups did not differ at different times [Table 3].
The results showed, at all times, no statistically significant difference in mean of diastolic blood pressure. This means that changes in diastolic blood pressure in both groups did not differ at different times [Table 4].

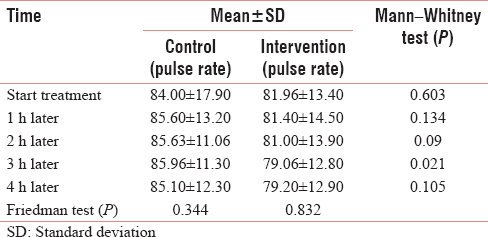
The results showed that, in all times but 3 h after the intervention, the mean heart rate in both groups was not statistically significant. This means that changes in pulse in both groups did not differ at different times [Table 5].
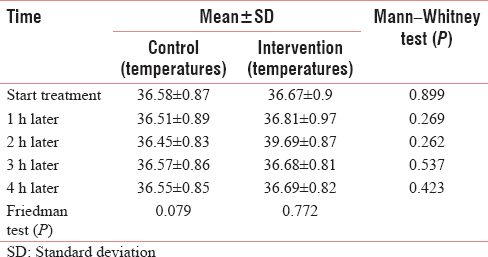
The results showed, at all times, no statistically significant difference in mean of temperature. This means that changes in temperature in both groups did not differ at different times [Table 6].
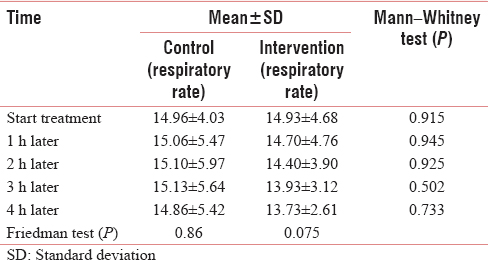
The results showed, at all times, no statistically significant difference in mean of respiratory rates. This means that changes in respiratory rates in both groups did not differ at different times [Table 7].
DISCUSSION
The results showed that the pain averages the control and experiment groups before intervention were 8.3 and 8.1, respectively, which show severe pain. This result conforms to the results by the previously done researches that revealed the high severity of orthopedic pains.[111213141516] Furthermore, the results of this paper showed that severity of pain in the two groups of experiment and control was not significantly different. Fractures in limbs result in severe pains were forced medical team to give narcotic drugs that make the treatment team to use narcotic analgesics.[111213141516]
The results showed that changes in pain severity in the intervention group have significant statistical differences at different times; over the time, the pain reduced significantly. These findings indicate the positive effect of the essential oil of orange on pain relief in the patients with orthopedic fractures, which are in line with the results by Lehrner on dental procedures.[35] Yip and Tam showed that aromatherapy and massage with orange oil and ginger can reduce knee arthritis pains,[28] conforming to the results of this paper. However, Małachowska et al. studied the pain from the Lancet to measure blood sugar in children with type I diabetes[3637] and obtained results different from the results in this paper; this difference may be due to difference in pains in orthopedic fractures and lancet. Ozgoli et al. showed that the orange oil can relive the pain in breasts caused by premenstrual syndrome.[29] Rashidi Fakari also showed that the orange oil can reduce labor pain, which is in line with the results of this paper.[25]
Another main objective of this paper was studying the effect of the orange oil on vital signs such as pulse rate, respiration, blood pressure, and body temperature in patients with fractured limbs admitted to the emergency ward. No significant difference was observed between the vital signs in the two groups at different times. Contrary to our results, Ja'farzade showed that inhalation of the orange oil decreased the heart rates in the children who had referred to dentist; this difference may be due to difference in the natures of dental procedures and fractures. Moreover, the atmosphere in the emergency ward, for example, crowdedness, long waits for surgery, and fear of the future may reduce the effect of the orange oil on the patients' vital signs. The limitation of this study was a lack of enough information about the complementary medicine by the patients, which could affect the results of effects of inhalation of the orange oil on the patients' vital signs in the study.
CONCLUSION
Aromatherapy with the essential oil of orange as a complementary medicine could relieve pain in patients with fractured limbs before surgery. It can lead to faster recovery and discharging of patients as well as reduce the costs of hospitalization. In this context, aromatherapy with the orange oil in patients with fractured limbs is recommended.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Optimising postoperative pain management in the ambulatory patient. Drugs. 2003;63:855-67.
- [Google Scholar]
- Evaluation of the effect of intravenous magnesium on acute postoperative pain in elective orthopedic surgeries of the lower limb. Pajoohandeh. 2006;11:149-52.
- [Google Scholar]
- Effect of postoperative analgesia on surgical outcome. Br J Anaesth. 2001;87:62-72.
- [Google Scholar]
- Epidural anesthesia and analgesia. their role in postoperative outcome. Anesthesiology. 1995;82:1474-506.
- [Google Scholar]
- Modification of responses to surgery by neural blockade. In: Cousins MJ, Bridenbaugh PO, eds. Neural Blockade in Clinical Anesthesia and Management of Pain Vol Vol. 11. (3rd ed). Philadelphia: Lippincott-Raven Publishers; 1998.
- [Google Scholar]
- Diaphragmatic shortening after thoracic surgery in humans. effects of mechanical ventilation and thoracic epidural anesthesia. Anesthesiology. 1993;79:654-65.
- [Google Scholar]
- Principle of Anesthesia and Critical Care. Isfahan: Mani Publicaton; 2001.
- Practice guidelines for acute pain management in the perioperative setting. A report by the american society of anesthesiologists task force on pain management, acute pain section. Anesthesiology. 1995;82:1071-81.
- [Google Scholar]
- Intrathecal midazolam regulates spinal AMPA receptor expression and function after nerve injury in rats. Brain Res. 2006;1123:80-8.
- [Google Scholar]
- The control of pain in peripheral tissue by opioids. N Engl J Med. 1995;332:1685-90.
- [Google Scholar]
- Effects of nonsteroidal antiinflammatory drugs on patient-controlled analgesia morphine side effects: Meta-analysis of randomized controlled trials. Anesthesiology. 2005;102:1249-60.
- [Google Scholar]
- A risk-benefit appraisal of injectable NSAIDs in the management of postoperative pain. Drug Saf. 1993;9:380-93.
- [Google Scholar]
- Efficacy of NSAIDs drugs in the management of postoperative pain. Drugs. 1992;44(Suppl 5):14-29.
- [Google Scholar]
- Child Health Nursing: Partnering with Children and Families (2nd ed). Pilladelphia: Prentice Hall; 2010.
- Basics of Anesthesia (5th ed). Philadelphia: Churchill Livingstone Elsvier; 2007. p. :112-22.
- Wong's Essentials of Pediatric Nursing (8th ed). Louis, MO: Mosby/Elsevier; 2009. p. :194-8.
- Which complementary and alternative therapies benefit which conditions? A survey of the opinions of 223 professional organizations. Complement Ther Med. 2001;9:178-85.
- [Google Scholar]
- Will aromatherapy be a useful treatment strategy for people with multiple sclerosis who experience pain? Complement Ther Nurs Midwifery. 2002;8:138-41.
- [Google Scholar]
- The effects of aromatherapy on painof labor in nulliparous women. J North Khorasan Univ Med Sci. 2013;5:363.
- [Google Scholar]
- Encyclopedia of Traditional Medicine Herbal (2nd ed). Tehran: Arjmand; 2005.
- Guidline of Herbal Medicine. Tehran: Islamic Azad University; 2005.
- An experimental study on the effectiveness of massage with aromatic ginger and orange essential oil for moderate-to-severe knee pain among the elderly in Hong Kong. Complement Ther Med. 2008;16:131-8.
- [Google Scholar]
- The effect oral of orange peel on the severity of symptoms of premenstrual syndrome, double-blind, placebo-controlled clinical trial. J Reprod Fertil. 2011;12:123-9.
- [Google Scholar]
- The effect of aromatherapy with orange essential oils on anxiety in patients undergoing hemodialysis. Q J Sabzevar Univ Med Sci. 2012;19:249-57.
- [Google Scholar]
- Measures of adult pain: Visual analog scale for pain (VAS pain), numeric rating scale for pain (NRS pain), mcGill pain questionnaire (MPQ), short-form mcGill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form-36 bodily pain scale (SF-36 BPS), and measure of intermittent and constant osteoarthritis pain (ICOAP) Arthritis Care Res (Hoboken). 2011;63(Suppl 11):S240-52.
- [Google Scholar]
- Measurement of chronic pain: A correlation study of verbal and nonverbal scales. J Behav Assess. 1981;3:63-9.
- [Google Scholar]
- Pain description and severity of chronic orofacial pain conditions. Aust Dent J. 1998;43:403-9.
- [Google Scholar]
- Correlation between visual analogue scale and short form of McGill questionnaire in patients with chronic low back pain. Qom Univ Medl Sci J. 2012;6:31-4.
- [Google Scholar]
- Ambient odor of orange in a dental office reduces anxiety and improves mood in female patients. Physiol Behav. 2000;71:83-6.
- [Google Scholar]
- Essential oils reduce autonomous response to pain sensation during self-monitoring of blood glucose among children with diabetes. J Pediatr Endocrinol Metab. 2016;29:47-53.
- [Google Scholar]
- Effect of aromatherapy with orange essential oil on salivary cortisol and pulse rate in children during dental treatment: A randomized controlled clinical trial. Adv Biomed Res. 2013;2:10.
- [Google Scholar]




