
Translate this page into:
Experience of Palliative Care Services at Tertiary Comprehensive Cancer Center during COVID-19 Lockdown Phase: An Analytical Original Study
Address for correspondence: Dr. Priti Sanghavi, Department of Pain and Palliative Medicine, Gujarat Cancer and Research Institute, Civil Hospital Campus, Asarwa, Ahmedabad - 380 016, Gujarat, India. E-mail: priti.sanghavi@gcriindia.org
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Recent pandemic Coronavirus disease 2019 has brought the whole world to a standstill. In India too, phases of the lockdown of the country were declared. This hampered the availability of essential health-care services to needy patients. With full emphasis on the pandemic, patients suffering from other diseases and palliative oncology patients requiring essential palliative care services were affected due to the shutting down of regular health-care services.
Aim:
In this study, we emphasize that in the middle of a pandemic, we need to continue serving the needs of palliative care patients, and simultaneously, necessary steps should be taken for the prevention of the spread of virus by following guidelines, training, support, and monitoring.
Materials and Methods:
In this study, we analyzed electronic medical record of 1161 patients who received palliative care from our institute in the first two lockdown periods, regarding their demographics, extent of travel, type of malignancy, and opioid utilization.
Results:
Of 1161 patients, male outnumbered female and the patient suffering from head-and-neck malignancy were in the maximum number (48.7%). Our essential opioids utilization rate was 34.2%, and patients who traveled from different states were 21.6%.
Conclusion:
During this pandemic, we cannot overlook the need for essential palliative care services. We can continue regular services with proper precautions as advised and by training the staff. Collaboration with different palliative centers across the country should be done to minimize patient movement.
Keywords
Coronavirus disease 2019
oncology
opioid
palliative care

INTRODUCTION
Coronavirus disease 2019 (COVID-19) has brought the world to the standstill with even developed countries finding it difficult to cope with the limited health resources. In India, the pandemic entered in January 2020. Little we knew that this unknown virus will lead to a total shutdown of the country with a population 1.3 billion, immensely affecting the whole community emotionally and financially.
During this lockdown, to manage health-care resources effectively, decisions to reschedule nonurgent outpatient visits, nonurgent elective surgeries, and elective procedures were taken globally.[12]
Our institute, despite being one of the biggest state cancer centers in Western India, also has to partially stop its elective treatment. Out of two hospital buildings, one is converted to a dedicated COVID-19 hospitals, and half of the workforce has been mobilized there. Due to this, collateral damage was done to oncology patients who were about to start their treatment or were undergoing some kind of treatment.
Lockdown, social distancing and need to manage symptoms of patients, and continuous supply of opioids in the current situation are some of the major issues we faced as pain and palliative care physicians.
Despite all these hurdles, we were able to provide symptom relief to our patients by various means such as teleconsultation and telephonic conversations with the patients along with hospital-based palliative care service.
In this analysis, we aim to analyze our data of outpatients, inpatients, emergency, and teleconsultations provided to palliative care patients. Apart from studying demographics, diagnosis, and opioid utilization, we also analyzed the precautions we took to prevent the transmission of COVID-19 and safeguard the health of our doctors, staff, and the patients.
There are lots of references[34] regarding palliative care to the COVID-19 patients, but we could find very few references[56] regarding essential palliative care services to oncology patients.
We intend to set certain guiding principles for the “Total Care” of palliative oncology patients in this era of pandemic, so that the dual purpose of alleviating sufferings, timely intervention along with the protection of our staff can be achieved maximally.
MATERIALS AND METHODS
This study was conducted in the department of pain and palliative medicine, tertiary comprehensive cancer center of Gujarat. All patients availing pain and palliative care service along with teleconsultation during the lockdown period from March 23, 2020, to May 3, 2020, were analyzed. After institutional review board permission, electronic medical records were used to retrieve data for demographic locations, extent of travel, types of cancer, and opioid utilization.
Statistical analysis
The retrieved data were tabulated and analyzed. The total number of patients is given in the tabulated form and analyzed in graphical form.
RESULTS
Total patients treated by pain and palliative care team were 1161 [Table 1]. Male and female distribution ratio was 780:381 [Table 1]. Of these 1161 patients, 36 patients were pediatric patients, and the youngest patient was 1-year-old. Ten patients were attended in the emergency room. Twelve patients required hospital admission for their symptoms control [Table 1].
| Total number of patients received palliative care service | 1161 |
| Number of patients visited palliative care OPD | 1066 |
| Teleconsultation for palliative care | 37 |
| Number of patients visited emergency room for palliative care | 10 |
| No indoor patients admitted under palliative medicine | 12 |
| Number of pediatric patients visited palliative care OPD | 36 |
| M:F | 780:381 |
OPD: Outpatient department
Maximum patients were from Ahmadabad (50.0%) followed by who traveled from other cities of Gujarat (28.3%). During this lockdown period, 251 patients (21.6%) were from other states. Of these, patients or caregivers were mostly traveled from Rajasthan – 77 (6.60%) followed by Uttar Pradesh – 74 (6.30%) and Madhya Pradesh – 70 (6.02%) [Figure 1]. Few patients, who were present in the city for their oncology treatment, were stuck due to lockdown.
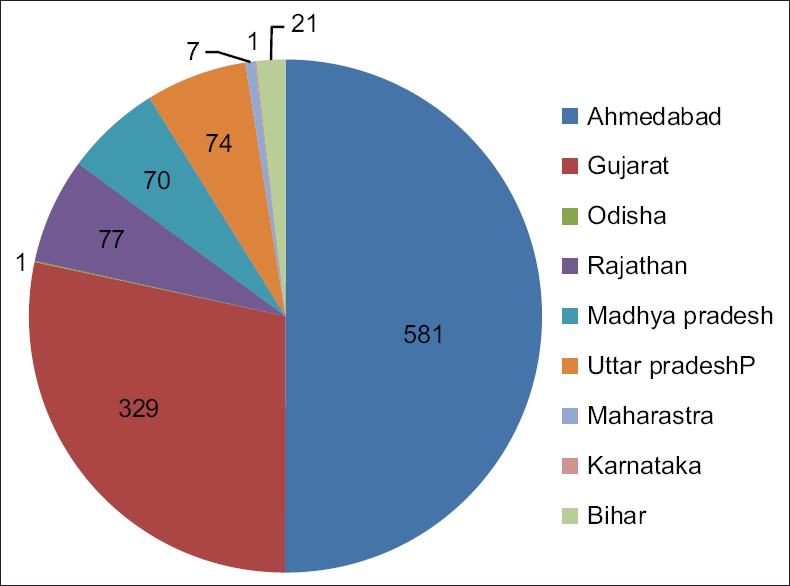
- Area-wise distribution of patients visiting palliative medicine outpatient department
Number of patients suffering from head-and-neck cancer were maximum (48.7%) followed by gastrointestinal and hepatobiliary (13.0%), breast (8.1%), lung (7.7%), gynecological malignancy (6.4%), bone cancer (4.8%), hematological malignancy (4.4%), urology (3.7%), and brain tumor (2.9%) [Figure 2].
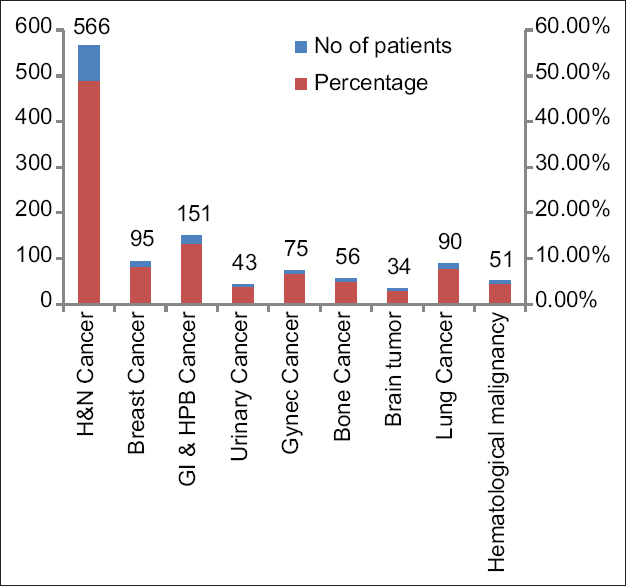
- Diagnosis-wise distribution of patients visiting palliative medicine outpatient department
Out of 1161 patients, 398 (34.2%) patients were prescribed as essential narcotics. Of these 398, most of the patients were prescribed morphine (95%) and fentanyl patch (4.5%), and only two patients (0.5%) were prescribed methadone [Table 2].
| Name of opioids | Number of prescriptions (%) |
|---|---|
| Tablet morphine | 378 (95) |
| Fentanyl patch | 18 (4.5) |
| Tablet/syrup methadone | 2 (0.5) |
| Total number of patients who received ENDs | 398 (34.2) |
ENDs: Essential narcotic drugs
DISCUSSION
India's first case was reported on January 30th in Kerala.[7] On the 1st day of lockdown 3.0, the figure increased enormously to ≥40,000.[8] During this lockdown, providing essential services to palliative oncology patients became exceedingly difficult. Despite these restrictions and with all the emphasis on COVID-19 patients, we were able to provide essential palliative care to 1161 patients through various means.
Many of these patients traveled far from other states. We found that people traveled to our center from as far as Karnataka and Odisha. Arranging the permission and vehicle to travel so far was a tedious, risky, and financially draining for the patient. These not only had increased risk to the patient owing to their immunocompromised state but also the accompanying person.
Most patients attending the outpatient department (OPD) were mostly suffering from head-and-neck cancer, as this is the most common malignancy we come across our state.[9]
The availability of opioids is not so widespread in India due to certain regulations.[10] Many patients traveled from far off distance due to the nonavailability of opioids in nearby centers.
However, still the fact is because of pandemic, we cannot overlook the need for oncology patients who are in severe distress. Hence, it becomes essential to prioritize the management of the patient as per the severity of the symptom.[6] As ESMO guideline,[6] priority of admission was given to patients suffering from severe distress such as intractable nausea/vomiting, refractory pain, or maggots infestation.
Patients were provided with an adequate supply of drugs, thus avoiding their need to travel frequently.[1] Telephonic consultation was provided for minor symptoms through our dedicated helpline number. Patients were also encouraged for telemedicine consultation.[111] We coordinated their regular supply of opioids from their nearby regional palliative care centers.[1213]
Due precautions were taken during OPD consultation, emergency consultation, and inpatient rounds to avoid virus transmission.[14] Training related to infection control, sanitization, Personal Protective Equipment (PPE) Kit, and the management of COVID-19 patients was made mandatory for all staff and doctors. This training was provided by the iGot.[15] Initial screening was done at the hospital building entrance. Patients were allowed inside the OPD with masks and were made to sit at a distance of 6 ft. Only one patient was allowed inside the room at a time to maintain the social distance. We could do this because of one-third workload of routine OPD. Washing of hands or the use of sanitizer was done every time after the consultation.[14]
Patients with severe symptoms who visited emergency were treated by taking proper universal precaution using PPE kit.[14]
We also emphasize on the “Total Care” of our staff by actively listening, supporting, and monitoring them.[1] By following the guidelines issued by the Government of India,[1415] we were not only able to treat the patients requiring palliative care services but also were successful in safeguarding our doctors and staff from unscrupulous exposure to the coronavirus.
CONCLUSION
By presenting this data, we want to emphasize that as this pandemic evolves over time, the need for continued palliative services for patients suffering from a life-limiting illness should not be under evaluated. Practical steps can be taken to ensure access to drugs (such as opioids) and protective equipment. We need to continue providing our services with proper precautions and consider greater use of telemedicine. We should collaborate with other regional centers across India so that the need for patients to travel for opioid prescriptions can be minimized. In this way, we can give requisite care to our patients and prevent cross infection by providing proper training and preparation across the health workforce.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Healthcare Facilities: Preparing for Community Transmission Coronavirus Disease 2019 (COVID-19). Available from: https://wwwcdcgov/coronavirus/2019-ncov/hcp/steps-to-preparehtml [Internet [Last cited 2020 May 12]
- Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323:1239-42.
- [Google Scholar]
- The key role of palliative care in response to the COVID-19 tsunami of suffering. Lancet. 2020;395:1467-9.
- [Google Scholar]
- Conservative management of COVID-19 patients-emergency palliative care in action. J Pain Symptom Manage 2020 pii: S0885-3924 (20) 30183-4
- [Google Scholar]
- Palliative care for patients with cancer in the COVID-19 Era. JAMA Oncol 2020:E1-2. doi:101001/jamaoncol20201938 Online ahead of print
- [Google Scholar]
- Palliative Care Prioritization during the COVID-19 Crisis; [Internet] 5th May 2020. Available from: https://wwwesmoorg/guidelines/cancer-patient-management-during-the-covid-19-pandemic/palliative-care-in-the-covid-19-era Cited 2020 May 05
- Available from: https://wwwindiatodayin/india/story/kerala-reports- first-confirmed-novel-coronavirus-case-in-india-1641593-2020-01-30 Last cited 2020 May 11
- Indian Council of Medical Research Three-Year Report of the PBCRs: 2012-2014; March, 2016
- Use of and barriers to access to opioid analgesics: A worldwide, regional, and national study. Lancet. 2016;387:1644-56.
- [Google Scholar]
- Telemedicine Practice Guidelines; 25 March 2020. Available from: https://mohfwgovin/ Last cited 2020 Mar 26
- PC Centre Directory of India Indian Association of Palliative Care. Available from: https://wwwpalliativecarein Last cited 2020 Mar 26
- Directory of Palliative Care Services. Available from: https://palliumindiaorg/resources/clinics/ Last cited 2020 Mar 23
- Preventive Measures to be Taken to Contain the Spread of Novel Coronavirus (COVID-19); 19th March 2020. Available from: https://mohfwgovin/ Last cited 2020 Mar 23
- Integrated Govt Online Training Portal for COVID 19; 11 April 2020. Available from: https://igotgovin/igot/explore-course Last cited 2020 Apr 14




