
Translate this page into:
Impact of Emotional Support on Serum Cortisol in Breast Cancer Patients
Address for correspondence: Mrs. Sampoornam Webster; E-mail: sampoornamwebster@yahoo.in
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Breast cancer is the most commonly occurring female cancer in the world. Research gap exists regarding emotional support for breast cancer patients.
Aim:
The main aim of this study was to compare the efficiency of Emotional Support- Focused Nurse directed Intervention on serum cortisol among arm I, II and III in breast cancer patients.
Methods:
The study was designed to compare the effectiveness of emotional support focused nurse directed intervention in terms of verbal, written and telephone basis on serum cortisol among breast cancer patients in Cancer Centre at Erode. Participants were randomly allocated by using Sequentially Numbered Opaque Sealed Envelope (SNOSE) method. 2 ml of blood samples were collected from 30 breast cancer patients who were selected randomly by adopting random number table, 10 in each experimental arm during evening at 18 hour; radioimmunoassay method was used to measure the level of serum cortisol before and after intervention. The intervention was given twice in a week for the duration of 30-45 minutes, in which early 20-30 minutes spares to express thoughts and feelings of the participants and subsequent 10-15 minutes for rendering informational support and later follow up session for the period of 1 month.
Results:
Emotional support was effective in reducing serum cortisol level among breast cancer patients. There was no statistically significant difference between arms on serum cortisol levels.
Conclusions:
Marginal differences were noted between posttest mean scores of serum cortisol among verbal, written and telephone arms. Further emotional support can be rendered according to the preference of the breast cancer patients.
Keywords
Breast cancer patients
Emotional support
Nursing intervention
Serum cortisol

INTRODUCTION
Cancer is one of the debilitating and life-threatening diseases with abnormal cell metamorphosis. It was first discovered in Egypt around 3000 BC. The causation of cancer is accounted on unknown determinants, pathogens, physical and chemical agents, dietary pattern, alcohol consumption, obesity, hormonal imbalance, and genetic link. The upsurge incidence of cancer predicted 15 million deaths by the year 2020.[1] In India, incidence of cancer is estimated approximately to be 2.5 million every year, which includes 8 lakh new cases and 5.5 lakh deaths.[2]
Breast cancer accounts for 23% of all newly occurring cancers in women worldwide and represents 13.7% of all cancer deaths. It is the most frequent cancer in both developed and developing region.[3] Higher incidence of breast cancer has been seen in developed countries such as Asia, Africa, and South America. It is estimated that 232,670 newly diagnosed breast cancer cases had 40,000 deaths at the United States in the year 2014.[4] The lowest incidence rates of breast cancer were found in most of the African countries. Breast cancer survival rates vary greatly in worldwide. The occurrence rates include 80% in North America, Sweden, and Japan. Around 60% were affected in the middle-income countries and below 40% from low-income countries.[5]
In India, breast cancer incidence has doubled in the past two decades. It is reported that one in 22 women is likely to suffer from breast cancer during her lifetime in India. Extensive widespread of breast cancer in India is a global public health burden and challenge. International Association of Cancer Research (2005) predicted 250,000 breast cancer cases will occur in India by the year 2015. An approximate number of newly diagnosed breast cancer cases in India will reach 2,00,000 by the year 2030.[6]
In 2015, the most commonly occurring cancers are breast cancer, lung and bronchus cancer, prostate cancer, colon and rectum cancer, bladder cancer, melanoma of the skin, non-Hodgkin lymphoma, thyroid cancer, kidney and renal pelvis cancer, endometrial cancer, leukemia, and pancreatic cancer.[4]
Breast cancer is the 2nd leading cause of death among women after lung cancer.
Stages and treatment of breast cancer lead to varied emotions such as fear, anxiety, anger, depression, despair, and helplessness for both patients and family members, Slevin et al.[7] Stress during cancer treatment causes severe emotional and psychological disturbances. Among all types of cancer, breast cancer has the greatest stress level due to treatment, stages, recurrence, life threat, disturbed body images, sexuality, fertility, and related issues femininity. Diagnosis and treatment of breast cancer is stressful that it could affect overall functioning. Stress has many dimensions such as emotional, psychological, and physical strain. Psychological stress causes emotional pain and upset. Emotional responses are unique and may vary over time. Stress management focuses on thoughts, emotions, schedules, environment, problem solving, self-care, rest, relaxation, biofeedback, strong supportive network, and cognitive restructuring.
Breast cancer patients encounter serious side effects which causes stress in the course of treatment. Breast cancer patients undergo emotional distress that elevates cortisol levels in the blood. Cortisol is considered as a stress marker and has an impact on the whole body. Stress hormone increases tumor size and rapid metastasis.[8]
Breast cancer survivors and women without breast cancer were tested for cortisol diurnal profile. Measurement of diurnal cortisol profile showed no significant difference between groups. In addition, subjective stress pattern evidenced no significant difference between groups. The diagnosis of breast cancer alters hypothalamic pituitary adrenal axis functioning.[9] Metastatic breast cancer women markedly showed a positive relationship between cortisol level, psychological changes, and subsequent traumatic occurrence related to the diagnosis of breast cancer. Posttraumatic stress also showed a positive relationship with cortisol.[10]
A study compared the diurnal cortisol slope with abdominal adiposity, perceived stress, social support, and explicit memory among metastatic breast cancer patients and healthy women. Result of this study showed metastatic breast cancer patients had increased cortisol rhythm than healthier women. Severity of the disease leads to higher cortisol levels. No relationship was determined between cortisol slope and cognitive functions of the patients. Healthier women showed exceeding waist circumference, meager explicit memory tasks, inadequate social support, and higher perceived stress.[11]
Breast cancer women were compared with healthy women on measures of salivary cortisol, urinary catecholamine, overnight urinary melatonin, sleep quality, stress, depression, anxiety, and mood disturbance. Women with breast cancer had higher levels of psychological disturbances compared to controls. No differences were found between groups on biological measures, except dopamine levels in controls. There was also no correlation between psychological and biological measures.[12]
Supportive care includes symptom control, psychological support, self-help, information, social support, rehabilitation, spiritual support, palliative care, and bereavement care. Emotional support offers confidence in breast cancer patients by building a relationship, exploring problems, analyzing, and resolving through decision making. Furthermore, emotional supports are essential to taper stress levels and promote quality of life in breast cancer patients. Patients who receive emotional support can adjust the situation even in worse condition. Informational support based on the needs of the cancer patients works a lot to adjust illness and can be retrieved from varied health personals. Nurses can provide informational support for breast cancer patients who desire and demands services. Providing information in appropriate time helps the cancer patients to cope illness, treatment, and situation.
Different methods of emotional support through verbal, written, telephone were not investigated in breast cancer patients. Choices should be given for the cancer patients to choose an appropriate emotional support. Literature has shown comparison between peer, face to face, and online community support in breast cancer patients. A study was conducted to compare written and verbal emotional disclosure on mood state and self concealment in breast cancer patients, Woods, and Kristine.[13] Still research gap exists with different modes of emotional support on stress and cortisol in breast cancer patients.
The focus of this present research lay on comparison of different modes of emotional support through verbal, written, telephone basis on cortisol in breast cancer patients.
MATERIALS AND METHODS
The three group pre- and post-test design was selected to compare the effectiveness of emotional support focused nurse directed intervention in terms of verbal, written, and telephone basis on serum cortisol among breast cancer patients in Cancer Center at Erode. Inclusion criteria were the breast cancer patients diagnosed with tumor in clinical Stage I to IV, under chemotherapy, radiation therapy, and surgical treatment. Those who were able to access telephone were included. Breast cancer patients with hearing impairment, those who were already having the habit of writing dairy and having mental illness were excluded from the study.
The sample included 30 breast cancer patients. Power analysis was used to estimate the sample size based on the findings of the pilot study with the assumption of 80% power. Using assuming verbal, written, and telephone arm besides the serum cortisol level P1 75%, P2 70%, P1 75%, P2 65%, P1 75%, and P2 60% correspondingly. The power calculation was based on alpha of 0.05 and expected mean effect size to meet the expected attrition rate at 10%. Difference between the group estimated that total participants were n = 30 breast cancer patients of which n = 10 women received verbal emotional support in experimental Arm I, ten received written emotional support in experimental Arm II, and ten received emotional support through telephone in experimental Arm III.
Totally 30 breast cancer patients, 10 in each arm were selected randomly during evening at 18 h to measure the serum cortisol level by adopting random number table. Proportionate stratification sampling was done based on I–IV Stages of breast cancer in each experimental arm. Participants were assigned randomly to either experimental Arm I (n = 10), or II (n = 10), or III (n = 10) so that the groups were balanced evenly according to the stages of breast cancer through propensity matching. Participants were randomly allocated using Sequentially Numbered Opaque Sealed Envelope (SNOSE) method. The steps involved in SNOSE method were as follows.
Step 1: Aluminumfoil was cut into thirty sheets with same width of envelope and twice its height. The carbon paper was cut into thirty envelope sized sheets, and standard size papers were cut into thirty sheets.
Step 2: The thirty standard size paper sheets were separated into four sets of 7 or 8 sheets based on cancer Stages I, II, III, and IV.
Step 3: On one set of 7 sheets in cancer Stage I, 3 sheets of treatment A (verbal), 2 sheets of treatment B (written), and 2 sheets of treatment C (telephone) were printed. Likewise, other sets of 8 sheets on cancer Stage I, 3 sheets of treatment A (verbal), 3 sheets of treatment B (written), and 2 sheets of treatment C (telephone) were prepared.
Step 4: Standard sized paper marked “treatment A” was folded to fit the envelope. One sheet of carbon paper was placed on top of the folded “treatment A” with carbon side facing the paper and on top of the carbon, one sheet of aluminum foil was placed and folded over both sides. Completed one was inserted into a blank envelope. Each envelope was sealed and signed with investigator's name in the pen over top of the envelope seal. Likewise, the “treatment B” and “treatment C” envelopes were prepared.
Step 5: In each cancer Stages I, II, III, and IV, 3 sealed “treatment A” envelops, 2 or 3 sealed “treatment B” envelops and 2 sealed “treatment C” envelops with total 7 or 8 envelopes were combined and shuffled as a deck of cards. A firm hand mark was made with number on the front of each envelope sequentially from 1 to 7 or 8 in pen. Based on cancer Stages I, II, III, and IV, 7 or 8 envelopes in each were placed into four separate plastic containers for use.
Step 6: Participants in breast cancer Stage I were made randomly to select an envelope and allocated to either verbal, written, or telephone intervention. Likewise, participants in breast cancer Stages II, III, and IV were made to select sealed, numbered envelopes and allocated to either verbal, written, or telephone intervention.
A volume of 2 ml of venous blood was collected from antecubital fossa by laboratory technicians and transferred to the ethylenediaminetetraacetic acid vacutainer. It was labeled with patient's name, age, and serial number. Throughout the procedure, aseptic measures were taken. The breast cancer patients cooperated very well throughout the procedure. The collected blood was kept in a cooling box with ice packs and transported to Hitech Diagnostic Centre NABL accredited laboratory holding certificate no M-0098 at Erode. In vitro radioimmunoassay method was used to measure the level of serum cortisol hormone during evening at 18 h. The lower and upper limit of low elevation of serum cortisol slope was measured as 15–25 mcg/Dl, respectively with manual scoring 1, likewise average elevation of serum cortisol slope was measured as 26–35 mcg/dL with manual scoring 2, and high elevation of serum cortisol slope was measured as 36–50 mcg/dL with manual scoring 3. Serum cortisol slope level was measured in terms of scores. Below 33% (1–10) were scored as low elevation of serum cortisol, 34–66% (11–20) were scored as average elevation of serum cortisol, and 67–100% (21–30) were scored as high elevation of serum cortisol. Parallel forms reliability was adopted to determine the accuracy ofin vitro radioimmunoassay method to measure the level of serum cortisol. The scores on the two different instruments were correlated to calculate the consistency between the two forms of the instrument, and the score was r = 0.89. The reliability coefficient for the parallel forms A (radioimmunoassay) and B (ELISA) to document serum cortisol variables indicated the high correlation; strong relationships were marked between both the forms. Because of cost effectiveness radioimmunoassay method was adopted for the study, Guber and Farag,[14] Stewart and Krone,[15] Tietz.[16]
Immediately after pretest the participants received emotional support focused nurse directed intervention which comprises one to one session. The session schedule was as follows [Table 1].

The intervention was given twice in a week for the duration of 30–45 min, in which early 20–30 min spares to express thoughts and feelings of the participants and subsequent 10–15 min for rendering informational support and later follow-up session for 1 month. Posttest was conducted using the same assessment techniques after the follow-up intervention for 1 month. The study was conducted after getting the approval from the Institutional Human Ethical Committee of Saveetha University (05/10/2012/IEC/SU; Dated 09 October 2012). Written permission was obtained from the chief medical officer, Erode cancer center dated on October 1, 2012, to conduct the study. Subject's right to withdraw/withhold the information was ensured before data collection. Patient telephone contact information was obtained from the subjects who participated in the study. The study was invasive for thirty breast cancer patients, 2 ml of blood was collected twice from the patients. It was ensured that safety and aseptic precautions would be taken into consideration during blood sample collection. It was assured that pre- and post-test serum cortisol estimation report would be given to the breast cancer patients. No risks were encountered. Confidentiality of the data was ensured throughout the study.
Descriptive, inferential, and nonparametric statistical analytic method was used to analyze and interpret the data. The data were expressed as frequency, percentage distribution, mean ± standard error. Paired t-test was used for estimating the effectiveness of emotional support in all experimental arms. One-way ANOVA was used to compare the effectiveness of emotional support among Arm I, II, and III. Post hoc multiple comparisons Tukey's test was performed to compare the mean difference among Arm I, II, and III. Tukey's honestly significant difference (HSD) test was aptly adopted for this study, as it has been constructed for pairs with equal number of samples. A probability of 0.05 or less was taken as statistically significant. Statistical Package for Social Science, PCT version 17 (SPSS Inc, Chicago) was used for analyzing the data.
RESULTS
Frequency and percentage distribution of pre- and post-test serum cortisol scores
Serum cortisol level was measured in experimental Arm I before treatment from 10 subjects, 2 (20%) marked with low elevation, 6 (60%) participants reported with average elevation, and 2 (20%) revealed high elevation of cortisol. After treatment experimental Arm I showed 4 (40%) with low elevation of serum cortisol, 5 (50%) participants measured with average elevation, and 1 (10%) marked with high elevation of cortisol slope [Table 2]. Serum cortisol slope was measured in experimental Arm II before treatment from 10 subjects, 1 (10%) reported with low elevation, 6 (60%) participants were noted with average elevation, and 3 (30%) marked high elevation. After treatment experimental Arm II depicted 1 (10%) participant with low elevation of serum cortisol, 8 (80%) measured with average elevation, and 1 (10%) marked with high elevation of cortisol slope [Table 2]. Serum cortisol was measured with experimental Arm III before treatment from 10 subjects, 1 (10%) marked with low elevation, 6 (60%) were noted with average elevation, and 3 (30%) measured with high elevation. After treatment experimental Arm III depicted 1 (10%) participant with low elevation of serum cortisol, 7 (70%) measured with average elevation, and 2 (20%) marked with high elevation of cortisol slope [Table 2].

Serum cortisol level before and after emotional support
Parallel comparison between mean, standard error concerning pretest serum cortisol scores with experimental Arm I showed 25.4 ± 2.46, furthermore posttest mean, standard error scores were 23.4 ± 2.41, respectively. Correspondingly comparison between mean, standard error of pretest serum cortisol scores with experimental Arm II marked 23 ± 1.95, moreover, posttest mean, standard error scores were 20.1 ± 1.87, respectively. Besides experimental Arm III reported the pretest mean, standard error serum cortisol scores 24 ± 1.93 and posttest mean, standard error scores were 21.5 ± 1.91 correspondingly. The outcomes were comparable to the significant difference between the mean pre- and post-test serum cortisol levels among experimental Arm I, II, and III. The mean score in all experimental arms decreased during the posttest and showed significant reduction in patient's serum cortisol level [Table 3].
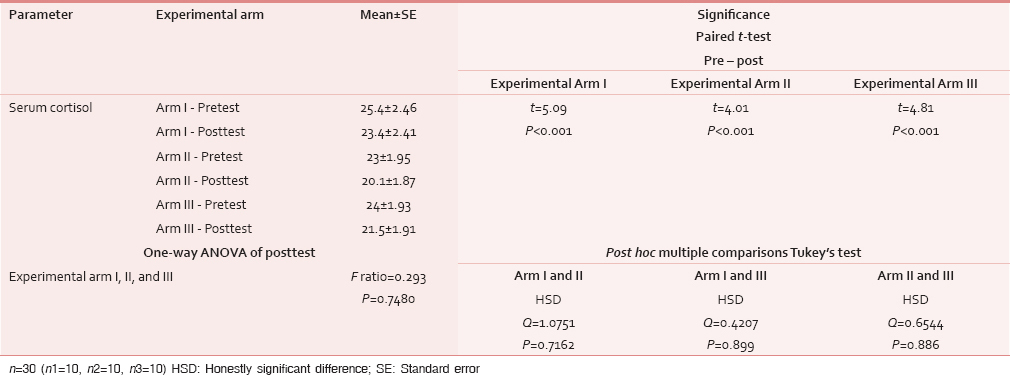
Paired t-test value of serum cortisol scores displayed in Table 3 showed statistical significance in experimental Arm I (t = 5.09), Arm II (t = 4.01), and Arm III (t = 4.81). One way ANOVA of posttest serum cortisol F ratio (0.2935) confined with experimental Arm I, II, and III showed no statistical significance [Table 3]. Post hoc multiple comparison Tukey's test failed to show the mean difference (Q = 1.0751) of serum cortisol between Arm I and II with no HSD between arms. Mean difference (Q = 0.4207) between Arm I and III demonstrated no HSD between arms. Likewise, mean difference (Q = 0.6544) between Arm II and III indicated no HSD constituted between arms. Conclusion drawn with no significant difference in the effectiveness of emotional support on serum cortisol bounded among the Arms I - verbal, Arm II – written, and Arm III - telephone. The posttest mean scores among Arm I (mean = 22.4), Arm II (mean = 20.1) and Arm III (mean = 21.5) showed slight difference [Table 3]. Based on posttest serum cortisol mean scores, written arm showed more efficiency compared to telephone and verbal arms.
DISCUSSION
Emotional support on serum cortisol in breast cancer patients
The study findings showed that most of the participants in experimental Arm I had average elevation of serum cortisol before and after treatment. Similar findings were reported with significant greater reductions in cortisol levels after cognitive behavior stress management program in breast cancer patients.[17] Serum cortisol slope was measured and found to be average in elevation before and after treatment in experimental Arm II, III. This conclusion is backing the research findings of intervention with cognitive behavioral stress management which showed reduced serum cortisol levels in the early stage of breast cancer patients.[18]
Significant mean differences were estimated in blood cortisol levels after the practice of Sudarshan Kriya and Pranayam in advanced stages of breast cancer at New Delhi, Kumar et al.[19] This study also showed that posttest serum cortisol scores were significantly lesser than the pretest scores in experimental Arm I, II, and III. Verbal, written, and telephone emotional support were statistically significant by reducing serum cortisol level within experimental arms. Research study supported that psychological intervention attenuated emotional distress and also decreased salivary cortisol levels in breast cancer patients, Stan et al.[20]
Two experimentations, body mind spirit, and educational session were compared for its effect on depression, meaning in life and salivary cortisol at home in the course of awakening. No significant difference noted with depression and meaning in life bounded by body mind spirit and educational session. Higher level of cortisol was measured in educational session than in body mind spirit. Body mind spirit contributed effectiveness on meaning in life and salivary cortisol for breast cancer survivors, Hsiao et al.[21] Outcome of various psychosocial interventions related to body mind spirit, supportive expressive, and social support self-help was tested on stress marker, psychological distress, mental adjustment, emotional control, and social support in breast cancer patients. Among 3 experiments Body Mind Spirit had paramount benefit in reducing salivary cortisol, psychological distress, negative mental adjustment, emotional control, and positive social support. Supportive-expressive participants, social support self-help group and control marked with statistically nonsignificance, Chan et al.[22]
Mindfulness meditation program was analyzed for its outcome on perceived stress, coping, salivary cortisol, and psychological stress response in patients with breast cancer. After intervening, significantly lower perceived stress, emotional coping, salivary cortisol, and psychological stress were marked, while controls had only marginal decline with the dependent variables, Kang and Oh.[23] Research examined the effect of yoga and brief supportive therapy in breast cancer outpatients on radiation therapy at Bangalore. Yoga treatment was more potent in reducing anxiety, depression, stress, and salivary cortisol level when compared with brief supportive therapy in early stage of breast cancer. Significant positive correlation was constituted between cortisol and anxiety, depression.[24] Supportive-expressive group therapy was given for the women with metastatic breast cancer. Intervention includes speaking time, repressive defensiveness, and anxiety affiliated with primary negative affect expression. Outcome showed that extreme cortisol slopes were related with reduced repressive defensiveness and increased primary negative affect expression.[25] Systematic review on randomized controlled trials reported the effectiveness of psychological intervention on biological variables among nonmetastatic breast cancer women. Psychological intervention influences cortisol and immune functional indicators such as lymphocyte proliferation and cytokine production.[26]
A cross-sectional study examined the relationships between interpersonal support, social support and mean and diurnal salivary cortisol slope in metastatic breast cancer women. Mean salivary cortisol inversely associated with interpersonal support. Social support does not associate with diurnal cortisol slope. Conclusions revealed that adequate social support were associated with lesser cortisol accumulation in metastatic breast cancer women.[27] Chinese breast cancer patients were examined to determine relationships between diurnal cortisol slope and perceived social support, sleep pattern. Association was found between higher cortisol levels and negative social support, and poor sleep quality.[28]
In this study, one-way ANOVA of serum cortisol F ratio confined between experimental Arms I, II, and III marked statistical nonsignificance. Effects of yoga based exercise were compared for its outcome between two groups. One-way ANCOVA was used for age, body mass index, cardiorespiratory capacity, and serum baseline marker. No significant differences were estimated between groups in breast cancer survivors.[29] Post hoc multiple comparisons Tukey's test was done in this study for serum cortisol. No HSDs were determined among Arms I, II, and III. Serum cortisol was used as stress marker in this study to draw objectivity in relation with stress levels in experimental Arms I, II, and III. Level of serum cortisol supports stress level in breast cancer patients with all experimental arms. Cortisol is considered as the stress hormone with an impact on breast cancer progression.[30] In this study, serum cortisol was checked only with 30 subjects due to its expensiveness.
Based on the findings of the study, the following conclusions were drawn. The study findings revealed that providing emotional support focused nurse directed intervention through verbal, written, and telephone modes reduced serum cortisol levels among breast cancer patients. There was no statistically significant difference among verbal, written, and telephone arms with emotional support on serum cortisol in breast cancer patients. Marginal differences were noted between posttest mean scores of serum cortisol among verbal, written, and telephone arms. Further emotional support can be rendered according to the preference of the breast cancer patients. It is recommended that emotional support can be provided by increasing the duration and frequency of intervention in breast cancer patients. Group setting intervention can be operated fairly and neutrally to identify the particular values of emotional support in breast cancer patients. Home based emotional support intervention can be rendered to recognize its effect on serum cortisol in breast cancer patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Opportunities for cancer epidemiology in developing countries. Nat Rev Cancer. 2004;4:909-17.
- [Google Scholar]
- Clinico pathological study and management of peripheral soft tissue tumours. J Clin Diagn Res. 2015;10:302-6.
- [Google Scholar]
- Trends in breast, ovarian and cervical cancer incidence in Mumbai, India over a 30-year period, 1976-2005: An age-period-cohort analysis. Br J Cancer. 2011;105:723-30.
- [Google Scholar]
- Cancer Statistics Review, 1975-2010. Bethesda: National Cancer Institute; 2013.
- Cancer survival in five continents: A worldwide population-based study (CONCORD) Lancet Oncol. 2008;9:730-56.
- [Google Scholar]
- Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893-917.
- [Google Scholar]
- Emotional support for cancer patients: What do patients really want? Br J Cancer. 1996;74:1275-9.
- [Google Scholar]
- Should supplemental antioxidant administration be avoided during chemotherapy and radiation therapy? J Natl Cancer Inst. 2008;100:773-83.
- [Google Scholar]
- Analysis of the cortisol diurnal rhythmicity and cortisol reactivity in long term breast cancer survivors. Breast Cancer Manag. 2014;3:465-76.
- [Google Scholar]
- Approach and avoidance coping: Diurnal cortisol rhythm in prostate cancer survivors. Psychoneuroendocrinology. 2014;49:182-6.
- [Google Scholar]
- Flattened cortisol rhythms in metastatic breast cancer patients. Psychoneuroendocrinology. 2004;29:1082-92.
- [Google Scholar]
- Associations among salivary cortisol, melatonin, catecholamines, sleep quality and stress in women with breast cancer and healthy controls. J Behav Med. 2007;30:45-58.
- [Google Scholar]
- The Effects of Written and Verbal Emotional Expression on Cancer Patients, Health Indiana University of Pennsylvania, Doctoral Thesis thesis
- Evaluation of endocrine function. In: McPherson RA, Pincus MR, eds. Henry's Clinical Diagnosis and Management by Laboratory Methods (22nd ed.). Philadelphia, PA: Elsevier Saunders; 2011. Ch. 24
- [Google Scholar]
- The adrenal cortex. In: Melmed S, Polonsky KS, Larsen PR, Kronenberg HM, eds. Williams Textbook of Endocrinology (12th ed). Philadelphia, PA: Elsevier Saunders; 2011. Ch. 15
- [Google Scholar]
- Textbook of Clinical Chemistry (3rd ed). Philadelphia: WB Saunders Co.; 1999. p. :1543-6.
- Stress management intervention reduces serum cortisol and increases relaxation during treatment for non metastatic breast cancer. Psychosom Med. 2008;70:1044-9.
- [Google Scholar]
- Cognitive-behavioral stress management reduces serum cortisol by enhancing benefit finding among women being treated for early stage breast cancer. Psychosom Med. 2000;62:304-8.
- [Google Scholar]
- Randomized controlled trial in advance stage breast cancer patients for the effectiveness on stress marker and pain through Sudarshan Kriya and Pranayam. Indian J Palliat Care. 2013;19:180-5.
- [Google Scholar]
- Breast cancer survivorship issues. Hematol Oncol Clin North Am. 2013;27:805-27, ix.
- [Google Scholar]
- The effects of psychotherapy on psychological well-being and diurnal cortisol patterns in breast cancer survivors. Psychother Psychosom. 2012;81:173-82.
- [Google Scholar]
- Arandomized controlled trial of psychosocial interventions using the psychophysiological framework for Chinese breast cancer patients. J Psychosoc Oncol. 2006;24:3-26.
- [Google Scholar]
- Effects of mindfulness meditation program on perceived stress, ways of coping, and stress response in breast cancer patients. J Korean Acad Nurs. 2012;42:161-70.
- [Google Scholar]
- Effects of a yoga program on cortisol rhythm and mood states in early breast cancer patients undergoing adjuvant radiotherapy: A randomized controlled trial. Integr Cancer Ther. 2009;8:37-46.
- [Google Scholar]
- Emotional expression and diurnal cortisol slope in women with metastatic breast cancer in supportive-expressive group therapy: A preliminary study. Biol Psychol. 2006;73:190-8.
- [Google Scholar]
- Psychological intervention and health outcomes among women treated for breast cancer: A review of stress pathways and biological mediators. Brain Behav Immun. 2008;23:159-66.
- [Google Scholar]
- Social support and salivary cortisol in women with metastatic breast cancer. Psychosom Med. 2000;62:337-45.
- [Google Scholar]
- The associations between diurnal cortisol patterns, self-perceived social support, and sleep behavior in Chinese breast cancer patients. Psychoneuroendocrinology. 2013;38:2337-42.
- [Google Scholar]
- Effects of six months of yoga on inflammatory serum markers prognostic of recurrence risk in breast cancer survivors. Springerplus. 2015;4:143.
- [Google Scholar]
- The glucocorticoid receptor mediates a survival signal in human mammary epithelial cells. Cancer Res. 2000;60:867-72.
- [Google Scholar]




