
Translate this page into:
Safety and Efficacy of Oral Transmucosal Fentanyl Citrate Compared to Morphine Sulphate Immediate Release Tablet in Management of Breakthrough Cancer Pain
Address for correspondence: Dr. Sanjaykumar H Maroo; E-mail: medicalservices@troikaapharma.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aim:
To compare the efficacy and safety of oral transmucosal fentanyl citrate (OTFC) and oral morphine in Indian patients with breakthrough episodes of cancer pain.
Materials and Methods:
In this randomized, open label, active controlled, clinical study, total 186 patients who regularly experienced 1-4 episodes of breakthrough cancer pain (BTCP) daily, over the persistent pain controlled by taking oral morphine 60 mg/day or its equivalent were randomized to receive either OTFC 200 mcg or oral morphine 10 mg for the treatment of BTCP for 3 days. Improvement in pain as determined by numerical rating scale (NRS) at 5, 15, 30, and 60 minutes of drug administration and percentage of BTCP episodes showing reduction in pain intensity by >33% at 15 minutes were primary efficacy endpoints. Secondary efficacy endpoints were requirement for rescue analgesia and global assessment by physician and patient. Data of both treatment groups were analysed by appropriate statistical test using software, STATISTICA, version 11.
Results:
Patients treated with OTFC experienced significantly greater improvement in pain intensity of breakthrough episodes compared to those treated with oral morphine at all assessment time points (P < 0.0001). 56% of breakthrough pain episodes treated with OTFC showed a greater than 33% reduction in pain intensity from baseline at 15 minutes compared to 39% episodes treated with oral morphine (P < 0.0001). Patient's and physician's global assessment favoured OTFC than oral morphine (P < 0.0001). Requirement of rescue analgesia in both the study groups was similar (P > 0.05). Both study drugs were well tolerated.
Conclusions:
OTFC was found to provide faster onset of analgesic effect than immediate release oral morphine in management of breakthrough cancer pain.
Keywords
Breakthrough cancer pain
Morphine
Numeric rating scale
Oral transmucosal fentanyl citrate

INTRODUCTION
Pain is one of the most common and troublesome symptoms of cancer.[1] At least two thirds of patients with advanced cancer report pain. Some degree of persistent pain is typically experienced most of the time which requires round the clock opioid treatment. Almost one half to two thirds of patients also experience breakthrough cancer pain (BTCP).[2]
BTCP is a transient increase in pain intensity over and above underlying background pain.[3] BTCP is characterized by an unpredictable, rapid onset of pain which lasts for an average duration of 30 minutes (ranges 15 minutes to 1 hour), generally self-limiting but severe in intensity.[3] Optimal management of BTCP therefore requires a medication with a rapid onset of analgesia and relatively short duration of action to match the course of episodes of BTCP.[4]
Currently, BTCP is managed by using oral supplemental opioid analgesia at a dose proportional to the total around-the-clock (ATC) opioid dose. This supplemental dose is given in addition to the continuous analgesic medication to manage pain flares. Out of currently available opioids for management of cancer pain, immediate-release oral morphine is commonly used for treatment of BTCP episodes, but its onset of effect does not match the rapid onset and short duration of most BTCP episodes. Other opioids like hydromorphone and oxycodone have similar limitation of slower onset of analgesia of 30-60 minutes. More recent recommendations have emphasized that orally administered opioids are not adequate for control of breakthrough pain of a short duration and rapid onset. Parenteral opioids may provide rapid onset of analgesia, but not always available particularly at home.[5]
Oral transmucosal fentanyl citrate (OTFC) is a novel, specifically designed intra-oral drug delivery to provide rapid analgesia for breakthrough pain episode. OTFC has been shown to have onset and peak of action similar to those of intravenous morphine for treatment of short duration breakthrough pain episode.[6] Absorption across the oral mucosa avoids first-pass metabolism, yielding a bioavailability substantially greater than oral administration and a peak plasma concentration within 22 minutes of administration.[2]
OTFC provides cost effective and easy to use treatment option for BTCP. OTFC is convenient for self administration by patients and does not require any nursing assistance or visit to hospital unlike parenteral opioids. OTFC has been used for treatment of BTCP with established efficacy and safety in USA and UK since many years. However, there is no data available for use of OTFC in Indian patients.
Therefore this study was designed to compare the efficacy and safety of OTFC and oral morphine tablet for the treatment of breakthrough episodes of cancer pain in Indian patients.
MATERIALS AND METHODS
This prospective, randomized, two arm, open label, active controlled, multicentric clinical study was conducted at pain and palliative care clinics of All India Institute of Medical Sciences (AIIMS), New Delhi; Tata Memorial Center, Mumbai; Kidwai Memorial Institute of Oncology, Bangalore; Rangadore Memorial Hospital, Bangalore and Basavatarakam Indo-American Cancer Hospital and Research Institute, Hyderabad. The study was approved by Institutional Ethics Committee of participating study centres. The study was registered in clinical trial registry-India (CTRI) prior to initiation of the study (CTRI Registration No: CTRI/2010/091/001179). The study was conducted in accordance with the Good Clinical Practice (GCP) guidelines issued by the Central Drugs Standard Control Organization (CDSCO), Ministry of Health, Government of India, and the ethical standards laid down in declaration of Helsinki 1964 and its later amendments; Ethical guidelines for biomedical research on human participants issued by Indian Council of Medical Research (2006), New Delhi.
Selection of participants
Patients visiting Out Patient Department (OPD) of cancer pain clinic, were screened for eligibility after taking written informed consent. Patients aged 18 or more, who experienced persistent moderate pain (having score of 5 or less on numeric rating scale, NRS) associated with cancer and having 1 to 4 episodes of breakthrough cancer pain (having score of 5 or more on NRS) per day while taking oral morphine 60 mg/day or its equivalent ATC dose to treat persistent pain for at least 7 days before enrolment were included in the study. Patient with known or suspected hypersensitivities and/or allergies to fentanyl or morphine; history of moderate to severe oral mucositis; history of convulsive disorder, head injury or comatose patients; history of neurological or psychiatric disorder; and history of abuse of alcohol or any other drug substance were excluded. The patients with history of either severe respiratory depression or severe obstructive lung conditions and those who have taken monoamine-oxidase inhibitors (MAOI) within the 2-week period prior to entering the study were excluded. Patients receiving radiotherapy or any other therapy, that in the investigator's opinion could alter pain or response to pain medication, were excluded. However, ongoing chemotherapy was allowed as per investigator's discretion in the study. The patients with uncontrolled or rapidly escalating pain and those in whom ATC medication might be expected to change during the course of the study as per the opinion of investigator were also excluded from the study. Pregnant and lactating women and women of child bearing age not practicing or not willing to use contraceptive were not included in the study.
Study treatment
Patients fulfilling the inclusion criteria were enrolled and randomized to receive either OTFC 200 mcg (Troyfentyl OTFC; Manufactured by Troikaa Pharmaceuticals Ltd, India) or oral morphine 10 mg tablet (Morphitroy tablet; Manufactured by Troikaa Pharmaceuticals Ltd, India) as and when required for the treatment of BTCP episodes for the period of 3 days. Separate simple randomization sequence, for each centre was generated by computer before start of the study with 1:1 allocation ratio in both the treatment groups.
Patients were hospitalized for study period of 3 days and monitored for occurrence of BTCP episodes. Patients were administered the assigned treatment whenever they had episode of BTCP during three days of study period. Patients in OTFC group were instructed to place OTFC unit in mouth between the cheek and lower gum, and move the drug unit from one side to the other using the handle. Patients were instructed to suck OTFC unit, not to chew. OTFC unit was consumed over a period of 15-minutes.
In comparator group, supplemental dose of oral morphine for break through pain was determined by the basal around the clock (ATC) oral morphine dosage. The supplemental dose for break through episodes of pain offered to the patient was 4-hour dose of the ATC oral morphine, based on recommendation of European Association for Palliative Care (EAPC).[7] In this study, all the patients were stabilized on 60 mg ATC oral morphine; hence the dose for breakthrough episodes of cancer pain for patients in oral morphine group was 10 mg.
Oral morphine 10 mg tablet was given as rescue medication in both the treatment groups if pain was not adequately relieved (NRS ≥ 4) after giving study medication. In OTFC group, rescue medication was given 15 minutes after the previous unit has been completed (30 minutes after the start of the previous unit). In morphine group, rescue analgesic was given if patients did not get adequate pain relief after 30-minutes of dosing.
No other adjuvant analgesics apart from study medication were allowed during the study. Medications considered necessary for the patient's concomitant diseases, which would not interfere with the study drug and evaluation of endpoints, were allowed as per investigator's discretion.
Efficacy assessment
Intensity of each breakthrough cancer pain episode was assessed at 0 (baseline, before dosing), 5, 15, 30, and 60 minutes after administrations of study drugs using NRS ranging from 0 to 10 (0 indicates “No pain”; 10 indicates “Worst possible pain”) over a study period of three days in each patient. At the end of the study, efficacy and safety of the study intervention was rated by physician and patient on global assessment categorical scale (Excellent, Good, Fair, and Poor).
Primary efficacy endpoints were, improvement in pain as determined by difference between NRS measured at each time point (5, 15, 30 and 60 minutes of drug administration) and baseline; and percentage of breakthrough episodes showing reduction in pain intensity by >33% at 15 minutes of drug administration. Requirement for rescue analgesia during study period and global assessment by physician and patients were included as secondary end points.
Safety assessment
Any adverse event (AE) reported/observed during study period was recorded in case report form. Incidence of adverse events was compared between two groups.
Statistical analyses
Considering standard deviation (SD) of 1.4 for pain intensity on NRS,[8] 5% level of significance (α = 0.05), a power of 80% to detect a clinically significant difference of 0.68 between the two groups, the required sample size was 90 patients per group. Considering a dropout rate of 10%, total sample size would be 100 patients per group. Sample size was derived using software, PS Power and Sample Size Calculations Program (version 3). Quantitative data were presented as mean ± SD, whereas categorical data were expressed as absolute number/proportion of patients. Quantitative data of both the treatment groups were analyzed by unpaired “t” test or Mann Whitney test based on the distribution of data. Chi-square test or fisher exact test was used to compare the categorical data of both the treatment groups. P value of less than 0.05 was considered as statistically significant difference between both the treatment groups. All statistical analyses were performed using software, STATISTICA, version 11. StatSoft, Inc. (2012).
RESULTS
Out of 237 patients screened, 186 patients satisfied the inclusion and exclusion criteria and enrolled in the study (95 patients in OTFC group; 91 patients in oral morphine group). Reasons for screen failure were patient receiving radiotherapy, had moderate to severe oral mucositis or were not stabilized on 60 mg of morphine 7 days before enrolment. All 186 patients completed the study and were subjected to statistical analysis [Figure 1]. Four hundred and forty-seven episodes of breakthrough pain were reported in OTFC group and 498 episodes reported in oral morphine group. Demographic and baseline characteristics (Pain intensity for persistence pain and breakthrough episodes) were similar in both treatment groups [Table 1].
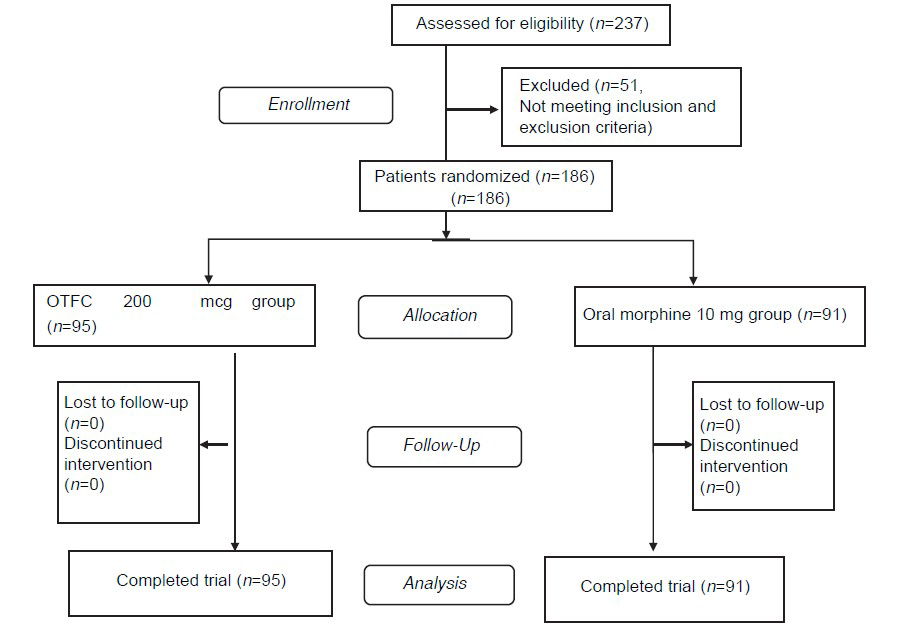
- Patient disposition flow chart (n is the number of patients)

Primary efficacy variables
Both treatments showed improvement in pain intensity on NRS from the baseline. OTFC was found to have rapid onset of action with better pain relief at 15 minutes as compared to morphine tablets. Fifty-six percent of breakthrough pain episodes (251 out of 447) treated with OTFC showed a greater than 33% reduction in pain intensity from baseline at 15 minutes compared to 39% episodes (194 out of 498) treated with oral morphine (P < 0.0001). Patients treated with OTFC experienced significantly greater improvement in pain intensity of breakthrough episodes as compared to oral morphine at 5, 15, 30, and 60 minutes of administration of study drug [Table 2].

Secondary efficacy variables
Rescue medication was required in 2 out of 95 patients (2.1%) in OTFC group while none of the patients in morphine group required additional rescue medication (0%); however, the difference between both the groups was not significant (P = 0.16). Global assessments of treatment by patient and physician based on overall efficacy and safety were significantly more favourable toward OTFC as compared to oral morphine (P < 0.0001) [Table 3]. No expected or unexpected adverse events were observed or reported during study period in either group. OTFC and oral morphine were equally well tolerated throughout the study period.

DISCUSSION
Breakthrough cancer pain is exaggeration of pain that occurs on top of an otherwise stable pattern of controlled pain. The occurrence of breakthrough pain is associated with greater psychological suffering and pain related disability.[29] Inadequately treated BTCP leads to poor quality of life. The treatment of BTCP in hospitalised patients is easy and prompt due to availability of opioid injections and trained staff. However, most of the patients with cancer pain are treated at home with round the clock opioid analgesics. So any BTCP episode at home is treated with additional dose of immediate release oral morphine or other oral opioids. However, longer time of onset of action of these medications usually does not lead to adequate relief of acute breakthrough pain episodes. Moreover, duration of action of these medications may be too long for short lasting breakthrough pain episodes.
OTFC is a fentanyl-containing oral transmucosal drug delivery system which readily dissolves in mouth. Because fentanyl is a potent and highly lipophilic opioid drug, it is readily absorbed from the oral mucosa, rapidly crosses the blood brain barrier and provide rapid onset of analgesia.[2] Rapid distribution of fentanyl into tissues also allows a relatively short duration of action.[2] These properties of rapid onset and short duration make OTFC more suitable drug for treatment of acute onset and short lasting BTCP episodes.
A trial comparing OTFC and oral morphine has been conducted in western countries in which OTFC used in dose ranging from 200 mcg to 1,600 mcg found to provide superior efficacy as compared to oral morphine.[2] Efficacy of OTFC in Indian patients has not been studied for treatment of BTCP. The present study compared OTFC and oral morphine for management of BTCP in Indian patients receiving fixed scheduled opioid regimen. In the present study, the dose of OTFC was 200 mcg and morphine was 10 mg because the patients enrolled in the trial were stabilized on the dose of 60 mg morphine or equivalent morphine in 24 hours.
In our study, OTFC and oral morphine both relieved the pain of breakthrough pain episode in cancer patients. OTFC was found to have rapid onset of action with better pain relief at 15 minutes as compared to morphine tablets. Fifty-six percent of breakthrough pain episodes treated with OTFC showed a greater than 33% reduction in pain intensity from baseline at 15 minutes compared to 39% episodes treated with oral morphine, implying faster onset of action with OTFC. Patients treated with OTFC experienced significant reduction in pain intensity of breakthrough episodes compared to oral morphine at 5, 15, 30, and 60 minutes of study drug administration. Our results were in line with the evidences which suggest that OTFC has a more rapid onset of action than oral opioids.
Our results are consistent with Coluzzi PH et al.[2] evaluating efficacy and safety of OTFC and oral morphine for management of breakthrough pain in patients receiving a fixed scheduled opioid regimen. The study also demonstrated significant improvement in pain intensity in patients treated with OTFC compared to oral morphine. In both studies, global assessment of treatment favoured OTFC and more patients opted to continue with OTFC than oral morphine following the study, suggesting better overall efficacy of OTFC compared to oral morphine.[2]
Requirement of rescue medication in both treatment groups were comparable. None of patient in either group experienced any adverse events during study period. Both drugs were found to be safe and tolerable in management of breakthrough cancer pain.
Dose of study medication in both arms needed to be individually titrated to a tolerable dose that could provide adequate analgesia in breakthrough cancer pain episodes with a titration strategy separate from that of the baseline cancer pain medication. Because of the availability of only one strength of OTFC, i.e. 200 mcg, titration of study medication was not possible in this study. Because of difference in formulation and route of administration in two treatment arms, study had been kept open label which might lead to biased results by patient/observer.
Although patient controlled analgesia (PCA) for management of BTCP episodes is widely popularized in western countries, majority of cancer patients in India cannot afford available resources of PCA. The breakthrough cancer pain is still being managed by oral morphine or similar oral opioids at home in India. This study is the first of its kind evaluating use of OTFC in Indian cancer patients which emphasizes benefits of OTFC use for “At Home” management of troublesome BTCP episodes in cancer patients in India. Future studies in outpatient basis are recommended to generate further data.
CONCLUSION
Based on results of the present study, it can be concluded that, OTFC is more effective and offers faster onset of analgesic effect with similar safety profile compared to immediate release oral morphine in managing breakthrough cancer pain. This new delivery system offers a highly effective alternative to commonly used oral morphine for management of breakthrough cancer pain.
Source of Support: Troikaa Pharmaceuticals Limited
Conflict of Interest: The study is sponsored by Troikaa Pharmaceuticals Ltd
REFERENCES
- Breakthrough cancer pain: Review of prevalence, characteristics and management. Indian J Palliat Care. 2009;15:14-8.
- [Google Scholar]
- Breakthrough cancer pain: A randomized trial comparing oral transmucosal fentanyl citrate (OTFC) and morphine sulfate immediate release (MSIR) Pain. 2001;91:123-30.
- [Google Scholar]
- Opioids for the management of breakthrough (episodic) pain in cancer patients. Cochrane Database Syst Rev :CD004311.
- [Google Scholar]
- Oral transmucosal fentanyl citrate use in chronic No cancer pain: A retrospective survey. Available from: http://www.crilifetree.com/media/abstracts/ORAL%20TRANSMUCOSAL%20FENTANYL%20CITRATE.pdf
- [Google Scholar]
- The use of rapid onset opioids for breakthrough cancer pain: The challenge of its dosing. Crit Rev Oncol Hematol. 2011;80:460-5.
- [Google Scholar]
- Oral transmucosal fentanyl citrate: Randomized, double-blinded, placebo-controlled trial for treatment of breakthrough pain in cancer patients. J Natl Cancer Inst. 1998;90:611-6.
- [Google Scholar]
- Opioids for the management of breakthrough cancer pain in adults: A systematic review undertaken as part of an EPCRC opioid guidelines project. Palliat Med. 2011;25:516-24.
- [Google Scholar]
- Oral transmucosal fentanyl citrate in the outpatient management of severe cancer pain crises: A retrospective case series. Clin J Pain. 2004;20:195-7.
- [Google Scholar]
- Breakthrough pain: Characteristics and impact in patients with cancer pain. Pain. 1999;81:129-34.
- [Google Scholar]




