
Translate this page into:
Analytical Study of Short- and Long-term Results of Home-based Palliative Care Services to Cancer Patients
Address for correspondence: Dr. Dhritiman Datta, Department of Oncology, Regional Cancer Centre, Agartala - 799 006, Tripura, India. E-mail: datta_dhritiman@yahoo.in
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aims and Object:
Identification and selection of patients suffering from terminal stage in bed ridden condition upto village level and to determine the type of palliative care need. Also to asses the effectiveness of the palliative care provided at the bed side.
Materials:
All registered patients under palliative care of Regional Cancer Centre, Agartala from 2014 April to 2016 March.
Methods:
A retrospective study. Ten teams comprising of doctors, nurses, pharmacists & Social Workers were trained and engaged in this study for symptom assessment and pain relief of palliative patients.
Results:
It is highly beneficial for the bed ridden & home bound cancer patients with improved quality of life due to regular home visits and medicine distribution by trained medical personnel. Short term benefits in symptom like pain, nausea & vomiting, retention of urine, constipation, bloating, fever etc. was dramatic after medication by palliative team. Patients also get relief as a result of repeated visit of palliative care team.
Conclusion:
Home based palliative care is beneficial for the bed ridden and home bound chronically ill patients including cancer patients. Bed ridden patients should be cared by palliative care team at least in every week.
Keywords
Northeast state
palliative care
quality of life

INTRODUCTION
Palliative care is defined by the World Health Organization as “An approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.”[1]
It is widely recognized that existing cancer treatments, in addition to the disease itself, can negatively impact the patient's physical, psychosocial, cognitive, and other aspects of well-being, which, in the aggregate, is called quality of life.[2] Some symptoms are more likely to cluster than others and thus may share a common cause (e.g., pain, fatigue, and depression).[3]
Recognition of symptom clusters should lead to better understanding of symptom pathophysiology, to targeted therapies, and improved quality of life. Using this approach may also reduce polypharmacy, lessen drug side effects, and produce pharmacoeconomic benefits.[4]
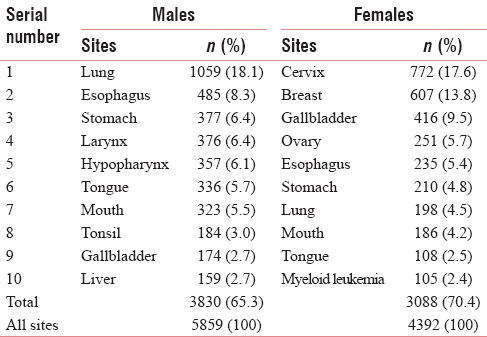
The population of Tripura, one of the Northeastern states in India is 3,673,917 according to census report 2011, of which male is 1,874,376 and female is 1,799,514. Cancer burden of Tripura as per population-based cancer registry reported malignant cases during 2010–2014 shows that the average annual specific crude rate of males and females is 61.4 and 47.9, respectively. The number of malignant cases reported in 2014 is 1208 males and 894 females with a ratio of 4:3. Leading sites of cancer for male population are lung, esophagus, hypopharynx, stomach, larynx, tongue, tonsil, mouth, etc. In female, cervix, breast, gallbladder, stomach, ovary, esophagus, lung, tongue, liver, and mouth are common in the state of Tripura.[5]
Around two-third patients present in very advanced stage of diseases. Morbidity and mortality are very high in this region of India. Palliative care plays a very important role to improve quality of life in end stage of disease.
The Home-Based Palliative Care Services of RCC, Agartala, throughout the state of Tripura launched on November 7, 2011, with the help of “Pallium India,” a Kerala-based NGO. The project completed successfully in November 2013. Then, home-based palliative care continued with the financial help from Indian Council of Medical Research (ICMR) and National Program for Palliative Care (NPPC).
Objectives of the study
-
To identify and select patient suffering from cancer at terminal stage in bedridden condition up to village level of Tripura (urban and rural)
-
To determine the type of palliative care need of the patient covering three districts, namely, (a) West Tripura, (b) Sepahijala, and (c) Khowai initially which later extended to other districts also
-
To assess the effectiveness of the palliative care on short- and long-term basis provided at the bedside.
MATERIALS AND METHODS
Materials
All registered patients under palliative care of RCC, Agartala, are taken from April 2014 to March 2016.
Methods
A retrospective study was carried out all from April 2014 to March 2016 with all palliative care patients registered under RCC, Agartala, Tripura. Ten teams comprising doctors, nurses, pharmacists, and social workers were trained for 10 days by Pallium India to conduct palliative care services in Tripura. RCC team and three district teams were engaged in this study for symptom assessment and pain relief of palliative care patients.
RESULTS
Home-based palliative care service is highly beneficial for the bedridden and homebound cancer patients. Most of the patients died due to advance stage of disease but with improved quality of life, such as healed fungated ulcer, relief from severe pain, respiratory distress, and other complications of advanced stage of cancer, due to regular home visit and medicine distribution by trained medical personnel.
The program benefits in a number of different ways. Patients felt respected, and cared for, and described feeling important and valued as people. Patients constantly expressed gratitude that because of the team's intervention, they no longer had to suffer with uncontrolled pain or live with poorly managed side effects or associated illness. Alongside the value of treatment being made available in their own home, reducing the emotionally and physically painful and economically costly travel to health centers, the program provided considerable value in meeting patients where they were with their families around them. Patients were treated as people leading their lives among their children, families, and household activities rather than as people with disease.
Effective pain relief delivered in a timely manner was noted by patients, volunteers, and staff as one of the most important contributions of the program. Previously, many patients had remained at home, too weak to travel to the local health centers or hospitals. Some patients described spending money they had borrowed for lengthy trips and treatments with traditional healers which had limited or no benefits until they met the home-based palliative care team.
Site-wise presentation of cancer in Tripura
Table 1 lists the ten leading sites of cancer in Tripura; for males, lung, esophagus, stomach, oropharyngeal region, gallbladder, and liver, and for females, cervix, breast, gallbladder, ovary, upper gastrointestinal, lung, and oral sites according to Population-Based Cancer Registry (PBCR), ICMR, Tripura. Patients usually present in advance stage of diseases.
It is seen that patients usually present in late stage due to delay in diagnosis or lack of awareness, reluctance, and resistance of existing health-care delivery system to guide these patients, nuclear family with no dependable person. Around 70% people belong to poor socioeconomic status. Many of them received traditional treatments such as homeopathy, ayurvedic, and other means of treatment.
The program had great societal impact and program implementing members were received by the community wholeheartedly. Political will and administrative support were extended to expand the program in every district. Now, the program is handed over to the National Health Mission (NHM) with expertise team to cover the entire eight districts under supervision of district health administrators. Teams are regularly visiting bedridden and homebound terminally ill chronic patients to relief them from sufferings. The aim is to see one such patients once in a week or at least in a month.
Home care visits done in different parts of Tripura during the years 2014–2016 show that more patients were visited in 2015, and in the months July–December, there are more number of patients visited [Figure 1].
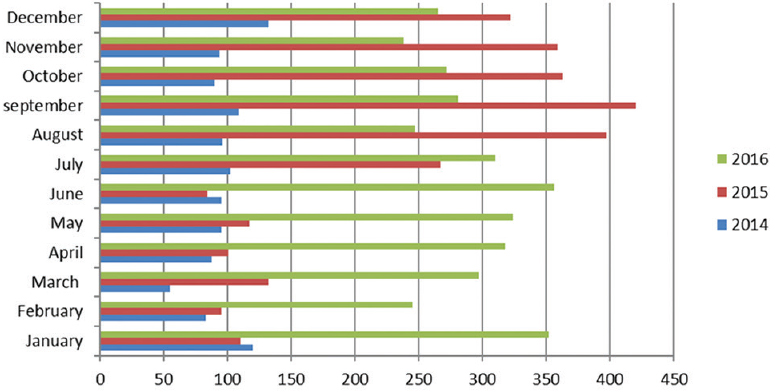
- Number of home visits throughout the state
Short-term benefits in symptoms such as pain, nausea, and vomiting, retention of urine, constipation, bloating, and fever were dramatic after medication by the home-based palliative care team. Each of the visits was a great relief to the patients and their relatives. Many of the patients lead to a quality life immediately after visit by the palliative team at the doorstep of the patients.
Patients got long-term relief from symptoms such as pain, general weakness, nausea, indigestion, depression, and sleeplessness (insomnia), as a result of repeated visit of palliative homebound team at a regular interval. Patients also could contact with palliative home care team by their or their relatives’ cell phones. This also gives them a psychological boost to have contact with palliative team.
Table 2 shows patients benefitted by palliative home care visit in 2014–2015 in West Tripura district were as follows: head and neck region cancer (19.36%), cervical cancer (13.1%), lung cancer (9.3%), and breast cancer (7.6%), and in Khowai district, 34.01% of patients were of head and neck region cancer, lung cancer (17.02%), esophageal cancer (12.76%), cervical cancer (10.63%), and breast cancer (4.26%). In Sephahijala district, 23.69% of patients were of head and neck region cancer, cervical cancer (14.45%), breast cancer (10.98%), lung cancer (9.25%), and esophageal cancer (6.36%).
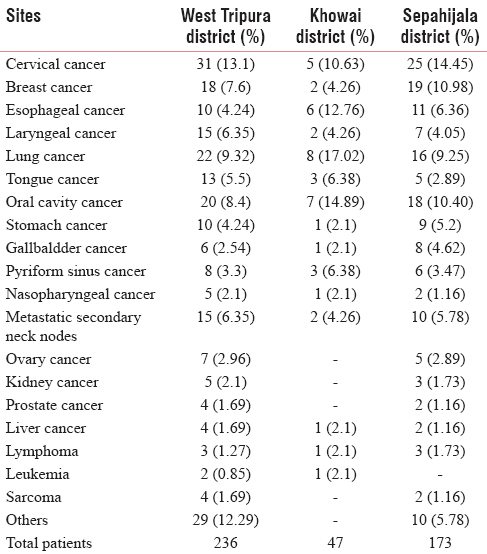
Head and neck and esophageal cancer patients suffered mainly from poor nutrition and pain. Other patients also suffered from pain and secondary infections.
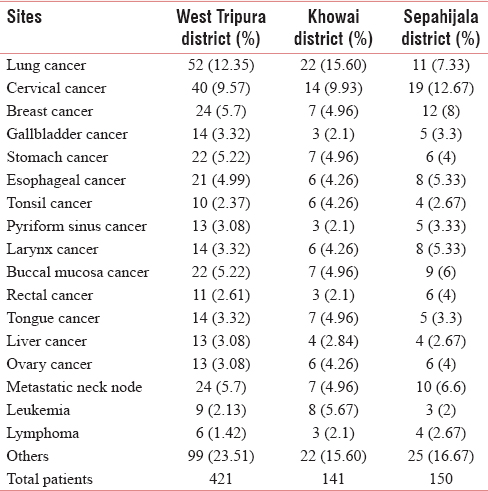
As per Table 3 in 2015–2016 as per visit of palliative team data, 23.02% of patients in West Tripura district were of head and neck region, whereas in Khowai and in Sepahijala, it was 25.5% and 27.23%, respectively. The next common cancer sites for West Tripura district were lung (12.35%), cervix (9.5%), breast (5.7%), stomach (5.22%), esophagus (4.99%), and gallbladder (3.32%), and for Khowai district, it was lung (15.60%), cervix (9.93%), leukemia (5.67%), breast (4.96%), and stomach (4.96%), and for Sepahijala district, next most common cancer sites were cervix (12.67%), breast (8%), lung (7.33%), and esophagus (5.33%).
Intensity of pain relieved by opioid (tablet morphine) as measured by opioid trial response scoring was satisfactory.
DISCUSSION
Palliative care provides medical and emotional services to the bedridden/homebound cancer patients at their door steps. Book for health personnel and NGOs are published in Bengali and English version.
In the state, one short survey was conducted by the registry staff of PBCR in the year 2012 and roughly identified 700 bedridden and homebound patients in Tripura, out of which approximately 3000 are cancer patients.
The management of the symptom of pain is only one component of a broad palliative care approach for cancer patients. The trained medical personnel used to look after the physical, psychosocial aspects of homebound/bedridden patients. Pain and other symptoms such as nausea, vomiting, cough, sleeplessness, sore mouth, breathlessness, constipation, and urinary symptoms are actively treated. At the same time, the emotional, social, and spiritual problems are addressed.
Medicines distributed to the palliative patients at their doorstep are tablet morphine, tricyclic antidepressants, nonsteroidal anti-inflammatory drugs, proton pump inhibitors, antibiotics, haloperidol, bisacodyl, cremaffin, bronchodilators, cough syrup, povidone iodine, turpentine oil, etc., by homebound palliative care team.
Bedridden patients are cared by palliative care team at least once in every week or at best within 10-day interval. Morphine is the only one of the drugs better use to relief pain. Any doctor or nurse can deliver palliative care provided they are trained. Although it is a medical problem, role of a layman is also there. Volunteers have a large role to play in it.
Palliative care is not only terminal care, but also the essence of palliative care is about providing a good quality of life. Research work done under the project in relation to age, sex, race, disease pattern, and geographical distribution of disease. Such research work will help to prepare proper plan for the better interest of cancer patients in the state.
Constraint
Bedridden patients should be cared by palliative care team at least in every week or at best within 10-day interval. At present, bedridden patients are seen once in 1 to 3 months in this hilly terrain of the country.
CONCLUSION
Results of Home based palliative care services gives a positive feedback towards the care for end stage disease sufferers. Considerable improvement in quality of life measures related to physical functions, satisfaction with treatment, emotional and financial conditions can be obtained by regular home care visit in end stage diseases. With continuous improvement of the palliative care and supportive system assessing the symptom burden, relieving the symptoms with adequate measures and ultimately improving the quality of life of these patients should be our objectives in health care delivery for incurable disease.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors would like to thank
ICMR, V. Ramalingaswami Bhawan, Ansari Nagar, Post Box No. 4911, New Delhi - 110 029, for providing logistics and data NPPC, NHM, MOHFW, Nirman Bhawan, New Delhi, Government of India Pallium India and Australia Palliative Alliance Doctors, nursing staff, and pharmacist attached to palliative care team of RCC, Agartala and three districts named West Tripura, Khowai, and Sepahijala, for their contribution in this study Prof. Raja Gopal, chairman, Pallium India, Kerala, for his contribution, guidance, and active support.
REFERENCES
- Available from: http://www.who.int/cancer/palliative/definition/en/
- Quality-of-life considerations in patients with advanced lung cancer: Effect of topotecan on symptom palliation and quality of life. Oncologist. 2004;9(Suppl 6):14-24.
- [Google Scholar]
- The Birmingham international workshop on supportive, palliative, and end-of-life care research. Cancer. 2006;107:874-81.
- [Google Scholar]
- Patterns of Cancer Incidence and Mortality in Tripura, A Five Year Report 2010-2014, Population Based Cancer Registry, Tripura, National Cancer Registry Programme (ICMR) 2016:22-8.
- [Google Scholar]




