
Translate this page into:
Association of Coping Styles with Quality of Life in Cancer Patients
Address for correspondence: Dr. Farid Arman; E-mail: farid.arman@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Backgrounds and Aim:
Cancer patients experience a high level of stress caused by the disease and treatment processes. Dealing with cancer using more beneficial coping styles can effectively improve the quality of life (QOL) and reduce the side effects of cancer, and it is treatment. In this study, we aimed to investigate the relationship between coping styles and QOL in cancer patients.
Methods:
The study was performed on 150 cancer patients (71 females and 79 males) admitted to the hospitals affiliated with Kermanshah University of Medical Sciences. Endler and Parker Coping Inventory for Stressful Situations, and World Health Organization's Quality of Life Questionnaire were used to evaluate their coping style and QOL, respectively.
Results:
The Present study showed in cancer patients being male, single, having higher salary and education, and lower age are related to higher QOL. Furthermore, in general, QOL of cancer patients was positively correlated with avoidant coping style (P < 0.05, r : 0.170) and negatively associated with emotion-focused coping styles (P < 0.01, r : −0.378).
Conclusion:
The results suggested that focusing on a patient's coping style, predominantly on an emotion-focused coping style, is essential to improve patient's QOL, and that patients possibly to employ a more emotion-oriented coping style should receive enough notice, particularly before discharge.
Keywords
Cancer
Psychiatry
Stress

INTRODUCTION
There is considerable evidence suggesting that cancer patients suffer from substantial and long-term psychological distress associated with different forms of cancer and its medical treatment.[1] Awareness of having a malignant life-threatening disease can obviously change patients’ lives. Cancers and any type of treatment may lead alteration in patients appearance. This issues can affect the quality of life (QOL), especially may reduce self-confidence, decrease self-esteem, having a problem with social interest, and finally may result in social withdrawal.[2] Studies have shown that psychological stress has a strong impact on accelerating the growth of various types of malignant tumors.[3] Hence, psychosocial management of adjustment problems experienced by people with cancer seems to be an obvious requirement for a more effective treatment of the disease.[4] Gynecological cancers have an impact on women's life. They can rise depression, anxiety, and impaired QOL.[5]
Recently, indicators of medical outcome for cancer patients have expanded to include QOL along with the survival rate, and accordingly, comprehensive patient care has focused on psychological as well as physical aspects. Cancer and it's treatment has a substantial impact on mental and social health and consequently, on QOL of patients.[6] Patient's psychological state and QOL should be considered in the light of factors such as the stage of disease and treatment process. Furthermore, it is important to recognize the relationship between psychological state/QOL and individual factors such as personality and coping style. Coping style, the individual cognitive response to stressors acknowledged by Folkman[7] in the 1980s, might function as a mediating variable controlling stress burden. On the other hand, coping style could conceivably be the cause or result of a patient's psychological state/QOL. There are three general styles of coping with stress: Problem-focused coping style, emotion-focused coping style, and avoidance style.[8]
Given the high costs that cancer imposes on patients and society, and considering the relationship between coping style and QOL in cancer patients, we can learn more effective coping styles for cancer patients to improve their QOL so that their psychological and even physical complications are reduced. The problem which we studied can be formulated in the following questions:
-
What styles of coping do patients with cancer adopt?
-
What is the state of QOL of patients with cancer?
Eventually, in this study our primary aims were an evaluation of coping styles and QOL in cancer patients, and our secondary aim was an investigation of the relationship between coping styles and QOL in cancer patients.
METHODS
In this study, patients with cancer who were referred to health centers affiliated with Kermanshah University of Medical Sciences (both inpatient and outpatient) were studied. Patients were selected randomly. Inclusion criteria entail: Over 18-year-old patients with diagnosed cancer that tended to participate in this study. Exclusion criteria include: Patients with any chronic physical or mental illness (other than cancer). Drug or psychotropic addiction were excluded, also patients who were in the end stage of cancer who could not communicate or interviews bothered them and patients who did not tend to collaborate. Demographic data including: Age, sex, marital status, salary, home location, education and cancer type was recorded via a self-structured questionnaire. Cancer stage (1 to 4) was discovered from patients records. Type of treatments at the time of the study was considered and recorded.
In the present study, Endler and Parker questionnaire was used to investigate patients stress coping styles and using World Health Organization's Quality of Life Questionnaire (WHOQOL-BREF), patient's QOL was evaluated. Two measures used in their translated and validated version. Endler and Parker questionnaire comprises 48 items on Likert scale from never (1) to very high (5). The inventory consists of three main scales: Task-oriented coping (TOC), emotion-oriented coping (EOC), and avoidance-oriented coping (AOC), with the last one with two subscales: Engagement in substitute activity and seeking for social relationships.[9]
Total QOL was measured using the Iranian version of the WHOQOL-BREF questionnaire which has been validated in our local Iranian population.[10]
The WHOQOL-BREF questionnaire consists of 26 questions and is based on a four-domain structure including:
-
Physical health activities of daily living, dependency on medical substances and medical aids, energy and fatigue, mobility, pain and discomfort, and sleep and rest
-
Psychological body image and appearance, negative feelings, positive feelings, self-esteem, spirituality/religion/personal beliefs, and thinking, learning, memory, and concentration
-
Social and personal relationships, social support, and sexual activity and
-
Environmental, including financial resources, freedom, physical safety and security, health and social care.
The scores ranged from 24 to 120 for the total QOL and 7–35 for the physical health, 6–30 for the psychological health, 3–15 for the social relationships, and 8–40 for the environment domains. Higher scores indicate better QOL.
Data analysis was performed by SPSS software V18 (Inc. chicago, USA) using descriptive statistics; correlation test was used to determine the correlation between QOL and various copying styles. Chi-square test was used to compare ratios for instance percentages; Student's t-test was used to compare the mean value of two quantitative group data and analysis of variance to compare averages between more than two groups. P < 0.05 was considered as significant.
RESULTS
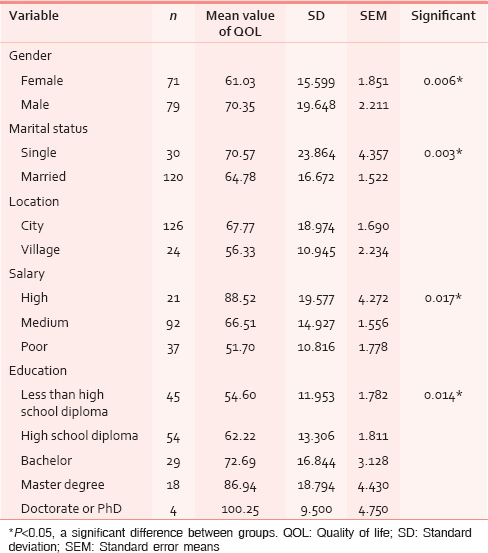
In the present study, 150 patients with cancer (71 females and 79 males) were investigated. Mean age of participants was 40.87 ± 11.46. 83 patients were in the young group (20–39 years), 60 in the middle-aged group (40–59 years) and seven in the elderly group (above 60 years). As shown in Table 1, 80% of patients (n = 120) were single and 20% (n = 30) were married. In the case of salary, 13.5% were in the high-salary group, 59.0% with medium-salary, and 23.7% had low salary. 80.8% of patients lived in city and 19.2% in the village. The most observed cancer type was breast cancer, and the least was uterus cancer [Table 2]. Our study showed 17.3% of cancer patients were in stage 1, 50.0% were in stage 2, 23.7% in stage 3, and 4.5% in stage 4.

About 44.2% of patients were undergone radiotherapy; 73.7% were undergone chemotherapy, and 68.6% were undergone surgery operations. There was no relationship between the type of treatment and copying style.
According to oncologist prescription, 4.5% of patients who were in stage 4 of cancer and were considered end stage just have received palliative cares and other patients have received both of curative and palliative cares.
As illustrated in Table 1, mean value of QOL was significantly higher in men than in women (P = 0.006), It was also significantly higher in single patients than in married ones (P = 0.003).
Furthermore, there was a significant relationship between QOL and salary; it was higher in patients with high income (P = 0.017). Age had a significant negative correlation with QOL (P = 0.034, r = −0.174). Furthermore, higher education showed a significant positive association with QOL (P = 0.014). There was a significant relationship between QOL and cancer type (P = 0.00).
Testis cancer group had the highest mean value of QOL while patients with uterus cancer showed the lowest mean value of QOL [Table 2], (P = 0.000). Comparing different therapeutic methods, the surgery caused a significant difference in QOL of patients while such difference was not observed in the other methods including chemotherapy and radiotherapy [Table 3]. Regarding the impact of stage of the disease on the QOL of patients, the only significant difference was observed in patients with stage 3 of cancer with patients in stages 1 and 2, as illustrated in Table 4.


Statistical analysis showed copying type was significantly associated with cancer type (P = 0.028), [Figure 1]. As it is depicted in the graph, patients with leukemia, ovary, uterus, lung, and colon cancer used problem-based copying type more than other copying types, while in breast and skin cancer, employment of problem and emotion-based copying types was more than avoidant copying style. Patients with bone and testis cancer employed avoidant copying style more than other types.

- Association between cancer type and copying type in cancer patients
There was not any significant association between copying type and income (P = 0.33), but patients with medium salary used problem-based copying type more than other patients [Figure 2].

- Association between salary and copying style in cancer patients
The results also showed that QOL of cancer patients have a positive correlation with avoidant coping style (P = 0.038, r: 0.170), while there was a significant negative association between emotion-focused coping styles and QOL (P = 0.000, r: −0.378), [Table 5]. Both in women and men, no significant correlation was found between QOL and problem-focused and avoidant coping styles, but QOL and emotion-focused coping style had a significant negative relationship (women: P = 0.000, r: −0.532, men: P = 0.027, r: −0.249) [Table 5].

In young adults (20–39 years), a significant negative relationship was observed between QOL and both problem-focused coping style (P = 0.012, r: −0.275) and emotion-focused coping style (P = 0.000, r: −0.423). The relationship between QOL and avoidance coping style was not significant. In the middle-aged group (40–59 years) QOL was significantly associated with problem-focused coping style (P = 0.012, r: 0.925), also a significant positive relationship was found with avoidant coping style (P = 0.008, r: 0.341). A significant negative relation with emotion-focused coping style also was observed (P < 0.01, r: −0.423). In the elderly group (over 60-year-old, 7 cases), QOL and problem-focused style were positively correlated (P = 0.034, r: 0.793). The correlations of QOL with emotion-focused and avoidant coping styles were not significant (P > 0.05), [Table 5].
DISCUSSION
Present study showed QOL in men was significantly higher than that in women. It also showed in single patients and those with a higher salary; QOL was significantly higher than that in other patients. Furthermore, age had a significant positive correlation with QOL. Regarding literature, in several studies like those of Aksnes et al.[11] bone cancer patients and Hashimoto et al.[12] arthritis, perceived health-related quality of life (HRQoL) were similarly found higher QOL in male than female patients. Chang et al.[1314] in a cross-sectional study, investigated gender impacts on HRQoL and related factors of postoperative lung-cancer patients. They also showed male participants had better physical, role, emotional, and cognitive functioning, so they had higher QOL. However, they showed married patients had significantly higher QOL, which is not in accordance with our findings. Similar to our study, Ferrel et al.[14] demonstrated income is positively associated with QOL[14] and in another study it has been reported that QOL of cancer patients get worse with age.[15]
One of the contributing factors of lower QOL in cancer patients can be a high prevalence of anxiety in these patients. Though Rodi et al.[16] reported a weak significant negative correlation between anxiety score and total QOL among prostate cancer patients. Furthermore, in another study it has been demonstrated that stress can be negatively correlated with QOL.[17]
We used the “Endler and Parker” and WHOQOL-BREF questionnaires to assess coping styles and QOL among cancer patients, showing that the emotion-focused coping style, in particular, were related to QOL, so that patients tending to use this coping style more probably experienced lower QOL than others. Young adults (20–39 years) with problem-focused coping style and emotion-focused coping style showed significantly lower QOL. In the middle-aged group (40–59 years), QOL was significantly higher in those with avoidance and problem-focused coping style, and lower in patients with emotion-focused coping style. Moreover, in the elderly group (over 60 years), the only positive correlation between QOL and problem-focused coping style was significant.
The results of this study showed there was a significant negative association between QOL and emotion-focused coping style in both women and men. However, there was no significant association between avoidance and problem-focused coping styles with QOL in both sexes. In a study, on gender differences in stress and coping styles, Matud[18] reported compared to men, women used more emotional and avoidant coping styles, and their coping style was more emotion-focused. In a review article on cancer patients, Baider and Bengel[19] revealed women initiate and communicate emotions while men try to avoid or withdraw from feelings and emotional demands. There is a trend toward expressiveness in women and instrumentality in men. Several studies have shown in chronic diseases; patients used positive and problem-focused coping styles less than other copying styles.[20212223]
In a study, on 78 elderly patients (over 70 years) and 105 younger patients (40–60 years) with carcinoma of the oral cavity and pharynx, Derks et al.[24] reported younger patients often use more active coping styles while older patients used religious coping styles in all assessments. In both groups, avoidant coping style was associated with more depressive symptoms. A study on 131 cancer patients in India has shown that the level of QOL in a patient with cancer were increased by chemotherapy treatment.[25]
As we have mentioned above, in young adults we observed those with problem-focused coping style and emotion-focused coping style showed significantly lower QOL. We did not find plenty of relevant references in literature, but according to Eslami et al. study[25] on congenital heart disease patients, the active problem-solving coping style was associated with never married marital status, parenthood, unemployment, higher level of anxiety/somatic symptoms, lower level of depressive symptoms, and better social support. From this study, we can interpret young adults with problem-solving copying style may experience some of these negative situations which can be a contributor to lower QOL among them. We recommend more precise studies be carried out to find its contributing factors.
Similar to our findings, a study in Japan[26] that aimed to assess coping styles in 85 patients with gastrointestinal cancer showed the higher the score of “EOC style,” the bigger the decline in QOL subscales.
Under the same conditions, the tendency to demonstrate EOC style (i.e., whether or not to respond emotionally) could in part establish QOL. A substitute view might be that the lower the QOL value becomes, the more emotionally a patient is possibly to react.[27] Therefore, it would appear more likely that a person with a trait of adopting a particular coping style would tend to experience a decline in QOL level as a result, rather than that a person would select a special coping style as a response to a preexisting low QOL. In a nutshell, in very stressful conditions, a person who had a negative coping style originally would have a more negative coping style, although a person who usually had a positive coping style was likely to take on a negative coping style.
Uehara et al.[28] studied the relationships between coping style assessed using the Coping Inventory for Stressful Situations and personality characteristic assessed using the Munich Personality Test, and reported that the TOC style was associated with “extraversion” and “frustration tolerance” personality, EOC style was related to “neuroticism,” “esoteric tendency” and “isolation tendency,” and AOC style was linked to “extraversion.” This recommends that people who tend to implement a more EOC style might be likely to assess their circumstances negatively rather than affirmatively.
With regard to coping style among cancer patients, Greer et al.[29] have reported a significant correlation between recurrence rate after 15 years and coping style assessed using mental adjustment to cancer and that between life expectancy and coping style. In addition, according to studies by Ho et al.[30] using Mini-Mental Adjustment to Cancer, Dunkel-Schetter et al.[31] using Ways of Coping-Cancer Version, and Akechi et al.[32] using the Japanese version of MAC, coping style could influence the psychological state in cancer patients. Therefore, the psychological aspect of QOL depends on the way in which individuals identify their disease state, treatment conditions, and associated circumstances and on how they deal with this. Hence, in the care of cancer patients, even if it is not probable to change a patient's coping style predominantly, we could optimize care by focusing on their individual coping style. As a result, we could not only discriminate whether or not the patient is in a risk group but also deliver and plan efficient and specific care by recognizing the patient's coping style. Moreover, such a psycho-educational approach might enable patients to acquire a more appropriate coping style.
This study had some limitations including: Lack of patient's tendency to participate in the study. We suggest more studies with greater sample size.
CONCLUSION
In general, emotion-focused coping style was associated with lower QOL in cancer patients. The results recommended that focusing on a patient's coping style, predominantly on an EOC style, is an important and that patients possibly to adopt a more EOC style should be given enough attention, particularly before discharge.
Source of Support: No.
Conflict of Interest: None declared.
REFERENCES
- Psychological sequelae of cancer diagnosis: A meta-analytical review of 58 studies after 1980. Psychosom Med. 1997;59:280-93.
- [Google Scholar]
- Quality of life in cancer patients with disfigurement due to cancer and its treatments. Indian J Palliat Care. 2011;17:184-90.
- [Google Scholar]
- Effects of therapeutic massage on the quality of life among patients with breast cancer during treatment. J Altern Complement Med. 2009;15:373-80.
- [Google Scholar]
- Effects of psychosocial interventions on quality of life in adult cancer patients: Meta analysis of 37 published controlled outcome studies. Patient Educ Couns. 2003;50:179-86.
- [Google Scholar]
- Baseline demographic profile and general health influencing the post-radiotherapy health related quality-of-life in women with gynaecological malignancy treated with pelvic irradiation. Indian J Palliat Care. 2013;19:186-91.
- [Google Scholar]
- Quality of life in cancer patients undergoing chemotherapy in a tertiary care center in malwa region of punjab. Indian J Palliat Care. 2014;20:116-22.
- [Google Scholar]
- Coping style and quality of life in elderly patients with vision disturbances. J Ophthalmol 2014 2014 584627
- [Google Scholar]
- Psychometric properties of the Iranian interview-administered version of the World Health Organization's Quality of Life Questionnaire (WHOQOL-BREF): A population-based study. BMC Health Serv Res. 2008;8:61.
- [Google Scholar]
- Young survivors of malignant bone tumours in the extremities: A comparative study of quality of life, fatigue and mental distress. Support Care Cancer. 2007;15:1087-96.
- [Google Scholar]
- A multicenter cross-sectional study on the Health Related Quality of Life of patients with rheumatoid arthritis using a revised Japanese version of the Arthritis Impact Measurement Scales Version 2 (AIMS 2), focusing on physical disability and its associative factors. Ryumachi. 2001;41:9-24.
- [Google Scholar]
- The effect of gender on health-related quality of life and related factors in post-lobectomy lung-cancer patients. Eur J Oncol Nurs 2014 Nov 05 Doi: 10.1016/j.ejon.2014.10.015. [Epub ahead of print]
- [Google Scholar]
- Quality of life and its related factors among iranian patients with metastatic gastrointestinal tract cancer: A cross-sectional study. Indian J Palliat Care. 2014;20:215-9.
- [Google Scholar]
- Anxiety status and its relationship with general health related quality of life among prostate cancer patients in two university hospitals in Kuala Lumpur, Malaysia. Iran J Public Health. 2013;42:240-8.
- [Google Scholar]
- The intermediary role of self-efficacy in relation with stress, glycosylated haemoglobin and health-related quality of life in patients with type 2 diabetes. Iran J Public Health. 2012;41:76-80.
- [Google Scholar]
- Cancer and the spouse: Gender-related differences in dealing with health care and illness. Crit Rev Oncol Hematol. 2001;40:115-23.
- [Google Scholar]
- A temporal framework for understanding the effects of stressful life events on inflammation in patients with multiple sclerosis. Brain Behav Immun. 2006;20:27-36.
- [Google Scholar]
- A replicated prospective investigation of life stress, coping, and depressive symptoms in multiple sclerosis. J Behav Med. 1997;20:433-45.
- [Google Scholar]
- Coping strategies, psychological variables and their relationship with quality of life in multiple sclerosis. Neurol Sci. 2009;30:15-20.
- [Google Scholar]
- Personality characteristics of multiple sclerosis patients: A Rorschach investigation. Clin Neurol Neurosurg. 2010;112:629-32.
- [Google Scholar]
- Differences in coping style and locus of control between older and younger patients with head and neck cancer. Clin Otolaryngol. 2005;30:186-92.
- [Google Scholar]
- Style of coping and its determinants in adults with congenital heart disease in a developing country. Congenit Heart Dis. 2014;9:349-60.
- [Google Scholar]
- Psychological state, quality of life, and coping style in patients with digestive cancer. Gen Hosp Psychiatry. 2005;27:125-32.
- [Google Scholar]
- Reliability and validity of the Japanese version of the coping inventory for stressful situations (CISS): A contribution to the cross-cultural studies of coping. Seishin Shinkeigaku Zasshi. 1993;95:602-20.
- [Google Scholar]
- Relationship between stress coping and personality in patients with major depressive disorder. Psychother Psychosom. 1999;68:26-30.
- [Google Scholar]
- Patients’ adjustment to cancer: The Mental Adjustment to Cancer (MAC) scale vs clinical ratings. J Psychosom Res. 1989;33:373-7.
- [Google Scholar]
- Psychometric properties of the Chinese version of the Mini-Mental Adjustment to Cancer (MINI-MAC) scale. Psychooncology. 2003;12:547-56.
- [Google Scholar]
- Psychometric properties of the Japanese version of the Mental Adjustment to Cancer (MAC) scale. Psychooncology. 2000;9:395-401.
- [Google Scholar]




