
Translate this page into:
Burden Experience of Caregivers of Acute Lymphoblastic Leukemia: Impact of Coping and Spirituality
Address for correspondence: Dr. Usha Chivukula, Centre for Health Psychology, University of Hyderabad, Prof. C R Rao, Gachibowli, Hyderabad - 500 046, Telangana, India. E-mail: chivukulausha@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
When a child is diagnosed with cancer the parents as caregivers experience severe anxiety, trauma, ambiguity, and grief. Caregivers of cancer patients thus deal with the management of their own psychological distress along with the child's illness.
Aim:
Coping plays a crucial role in improving the caregivers' physical and emotional well-being. Spirituality is an important means of consolation, strength, and emotional support during this phase. The present study aims to investigate the impact of coping and spirituality on caregiver burden.
Methods:
A total of 100 caregivers of children between the age group of 3–11 years, diagnosed with acute lymphoblastic leukemia were the participants of the study. The participants were recruited from cancer hospitals in Hyderabad. The study adopted a between-group design to find out if mothers and fathers differed in their coping strategies, spirituality, and caregiver burden. The study also adopted a correlation design to find the relationship between coping, spirituality, and caregiver burden. Descriptive statistics and multiple linear regression analysis were conducted to identify if coping and spirituality predict caregiver burden.
Results:
The results showed no significant difference in the burden experienced by both mothers and fathers; however, mothers and fathers used different coping strategies and differed on the dimensions of spirituality. The results of multiple linear regression indicated that dimensions of coping and spirituality were significant predictors of caregiver burden.
Conclusion:
Cancer in the child impacts the parent's burden but providing sufficient support and implementing effective coping strategies, will help in mitigating the intensity of caregiver burden. It is essential that the hospital authorities and policymakers understand that a professional health psychologist could be a liaison between the doctor, patient, and the caregiver in bringing down the levels of burden and psychological distress in caregivers as well as patients.
Keywords
Acute lymphoblastic leukemia
caregiver burden
coping
spirituality

INTRODUCTION
Cancer in children is not as common as in adults and only 1% of cancers are diagnosed in children.[1] Acute lymphoblastic leukemia (ALL) is the most commonly diagnosed cancer in children across the globe and constitutes 75%–80% of childhood acute leukemias in India.[2] The overall survival rate of ALL ranges from 45% to 81%, nevertheless, caregivers deal with the child's experience of prolonged and aggressive treatment and their own emotional distress. The trajectory of illness has an overwhelming impact on both the child and the caregiver. Moreover, a decline in the functional status of the patient results in higher burden and greater scope for the development of depressive symptoms in the caregivers.[3] A study conducted on parents of leukemia patients indicated that 85.8% of them showed signs of depression as an initial reaction to their child's diagnosis and 42.8% displayed anger and disturbances in family functioning following cancer diagnosis.[45] With complexities in the treatment process and the prognosis, the caregiver's role predominantly intensifies. Caregivers experience extreme stress; hence, the concern about their ability to cope with the responsibilities and demands of giving care is paramount.[6] As they try to adapt to the stressful situation, they employ both problem- focused and emotion-focused coping strategies.[7] A study done on caregivers of schizophrenic patients identified majority caregivers as using “mixed” type of coping mechanisms to deal with their stress which associated with caregiver burden, psychological morbidity, caregiving experience, social support, expressed emotions, quality of life, and psychopathology in patients.[8] Within the published literature from India, one study has identified that some of the most commonly used coping strategies by caregivers included acceptance, social support, problem-solving, and also involving in religious activities.[9]
Spirituality is an effective strategy to improve the quality of life, psychosocial adjustment to the treatment of cancer,[10] better maintenance of relationships between the caregiver and the recipient,[11] which indirectly decreases the caregiver distress,[12] decrease in the probability of poorer mental functioning within the caregivers,[13] and allows caregivers to feel positive about their caregiving role.[14] In a comparative study between caregivers of dementia and cancer patients, one of the major correlates for positive emotional state included the support received from the caregivers' religious faith.[15]
In the United States, according to the National Alliance for Caregiving report of 2015, 2.8 million individuals are caring for cancer patients.[16] Caregivers of cancer patients globally have received generous attention in the field of research and development of interventions due to their pivotal role in caring for the cancer patients. But unfortunately, their role has received very little attention in the published literature of India.[17] Caregivers are expected to shift their roles between managing day-to-day responsibilities, financial management, communicating with medical professionals, handling the medication and diet of patients, and managing the patient's psychological distress to name a few. In managing their role, they undergo severe health consequences which often takes a back seat.
Objectives
-
To determine if mothers and fathers of children suffering from ALL differ on coping, spirituality, and caregiver burden
-
To determine if there is a relationship between the dimensions of caregiver burden, coping, and spirituality among the caregivers of children suffering from ALL
-
To determine if coping and spirituality predict caregiver burden.
METHODS
Design
The present study adopted a between-group design to determine whether the caregivers, namely, mothers and fathers of children with ALL differ on coping, spirituality, and caregiver burden and their dimensions, followed by a correlational design to determine the relationship between the three variables. Multiple linear regression analysis were conducted to identify the predictors of caregiver burden.
Sample
A nonprobability purposive sampling method was used to select 100 participants (50 mothers and 50 fathers) from pronounced cancer hospitals located in Hyderabad city. The selected participants were primary caregivers (parents) of the children between the age group of 3–11 years, who were suffering from ALL. Caregivers of children who were in palliative care and/or those who received external care for their children such as a nanny or a babysitter were not included in the study.
Instruments
The brief cope
The brief cope was used to assess coping among caregivers.[18] It is a 28-item, self-report questionnaire consists of 14 subscales with two items under each: Self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, acceptance, religion, and self-blame. Scales are computed individually with no reversals of coding and no overall scoring. The reliability indicated a high Cronbach's alpha values ranging from 0.57 to 0.90.[18]
The spirituality scale
The spirituality scale was used to measure spirituality.[19] The scale has 23 items divided into three subscales: Self-discovery, relationships, and eco-awareness. Lowest and highest possible total score on this scale are 23 and 138, respectively. The lowest and highest possible scores on the subscale self-discovery are 4 and 24, respectively; on the subscale relationships the scores are 6 and 36, respectively, and on the subscale eco-awareness, the scores are 13 and 78, respectively. Reliability estimates ranged from 0.81 to 0.94 for the subscales.[19]
The caregiver burden inventory
The caregiver burden scale was used to measure the burden of caregivers.[20] The scale has 5 subscales: Time dependency, development, physical burden, social burden, and emotional burden. If the sum of the scores on all items is >36, it indicates a risk of “burning out” or higher burden, whereas if the scores are near or slightly above 24, it indicates a need to seek some form of respite care. The internal consistency reliability of each factor is 0.85 for time dependency, 0.85 for development, 0.86 for behavior, 0.73 for social burden, and 0.77 for emotional burden.[20]
Procedure
After seeking the permission from the cancer hospitals the caregivers were identified. Informed consent was given to them. Those who consented were given the information schedule after an initial rapport was established. The caregivers who met the criteria of the study were asked to complete the questionnaires. Written and oral instructions were given to them and they were asked to seek clarifications in case of doubts. The participants were debriefed and thanked after they completed the questionnaires.
Scoring and data analysis
The obtained data were entered into IBM SPSS, version 20.0 (2011) and analyzed using t-test, Pearson product–moment correlation, and multiple linear regression.
RESULTS
The results were analyzed to see the difference in coping, spirituality, and caregiver burden among mothers and fathers of children with ALL. The results also attempted to finding out if coping and spirituality predict caregiver burden.
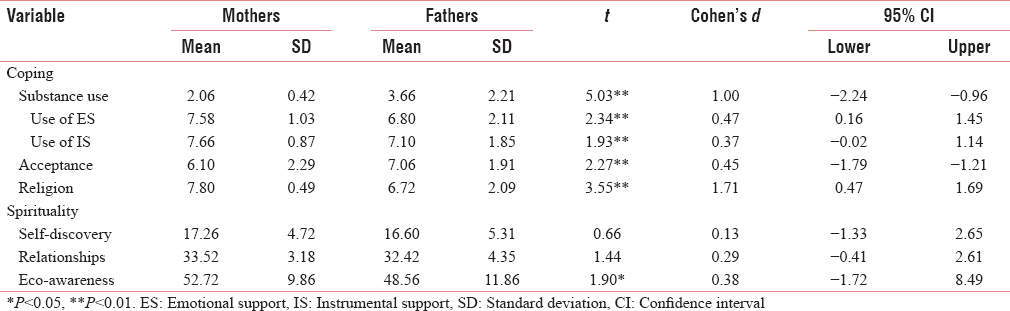
The results of independent t-test presented in Table 1 revealed that both groups of caregiver's, namely, mothers and fathers of children suffering from ALL did not differ significantly on caregiver burden indicating that regardless of the gender, both caregivers experience similar levels of caregiver burden, but a significant difference was found between these two groups on certain dimensions of coping and spirituality. The results revealed significant differences were observed between the two groups of caregivers on five dimensions of coping such as substance use (t = 5.03, P < 0.01) use of emotional support (t = 2.34, P < 0.01), use of instrumental support (t = 1.93, P < 0.01), acceptance (t = 2.27, P < 0.01), and religion (t = 3.55, P < 0.01). The mean differences among the dimensions of coping indicated that mothers use coping techniques such as emotional support, use of instrumental support and religion to a greater degree, on the other hand, fathers were found to use substance use and acceptance as coping strategies. It was also observed from Table 1 that mothers and fathers differed significantly on the eco-awareness dimension of spirituality. Mothers were found to be higher on the eco-awareness than the fathers. The above findings are diagrammatically represented in Figure 1. From Table 1, it may also be observed that the effect size was found to be high in case of substance abuse (Cohen's d = 1.00) and religion (Cohen's d = 1.71), whereas a medium effect size was observed in the dimensions of emotional support (Cohen's d = 0.47) and acceptance (Cohen's d = 0.45), while a low effect size was observed in case of instrumental support (Cohen's d = 0.07) and eco-friendliness dimension of spirituality (Cohen's d = 0.38).
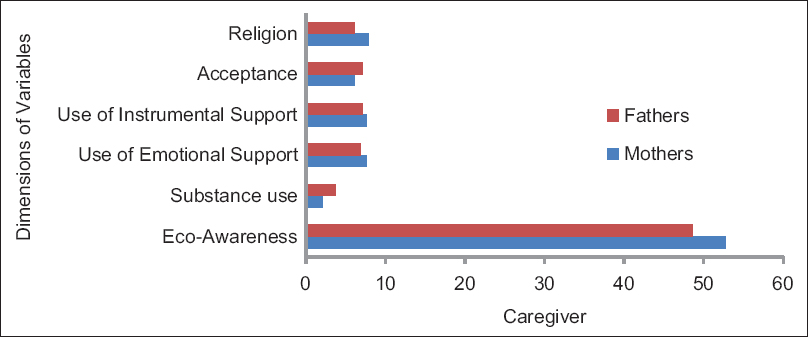
- Graph showing significant differences among mothers and fathers on some of the dimensions of Coping and Spirituality
The results of correlation presented in Table 2 indicated that there were significant relationships between the dimensions of the variables coping, spirituality, and caregiver burden among caregivers of children suffering from ALL. A multiple linear regression analysis was computed to determine the impact of coping and spirituality on caregiver burden.

From Table 3, it can be identified that the dimensions of coping contributed a significant proportion of variance on the dimensions of caregiver burden. The self-distraction dimension of coping contributed to 4% of variance in developmental burden, 17% variance in physical burden, and 4% variance in emotional burden dimensions of caregiver burden. Denial, another dimension of coping, had contributed 5% variance in developmental burden and 27% variance in physical burden dimensions of caregiver burden.
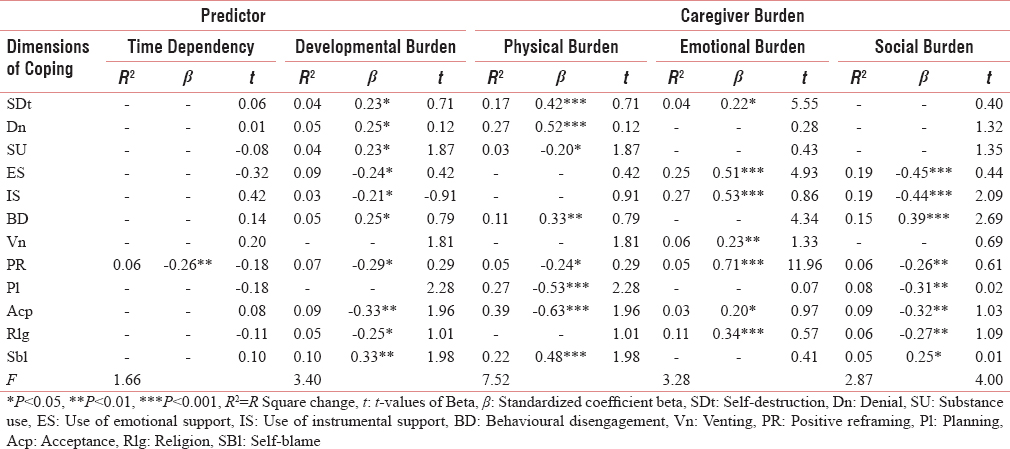
The substance use dimension of coping contributed to 4% variance in developmental burden and 3% variance in physical burden. The use of emotional support dimension of coping had also made a significant proportion of variance in the dimensions of caregiver burden. It contributed to 9% variance in developmental burden, 25% variance in emotional burden, and 19% variance in social burden. Similar to the use of emotional support, the use of instrumental support dimension of coping had contributed to 3% variance in developmental burden, 27% variance in emotional burden, and 19% variance in social burden dimensions of caregiver burden. The behavioral disengagement dimension of coping had contributed to 5% variance in developmental burden, 11% variance in physical burden, and 15% variance in social burden dimensions of coping.
Positive reframing was seen to be the only dimension of coping that contributed significant proportion of variance in all the dimensions of caregiver burden. Positive reframing contributed to 6% of variance in time-dependency, 7% variance in developmental burden, 5% variance in physical burden, 5% variance in emotional burden, and 6% variance in social burden dimensions of caregiver burden.
Planning, another dimension of coping, had contributed to 27% of variance in physical burden and 8% of variance in social burden dimensions of caregiver burden. The acceptance dimension of coping had also made significant contributions to the dimensions of caregiver burden. It had contributed to 9% variance in developmental burden, 39% variance in physical burden, 3% variance in emotional burden, and 9% variance in social burden dimensions of caregiver burden.
The religion dimension of coping contributed to 5% variance in developmental burden, 11% variance in emotional burden, and 6% variance in social burden dimensions of coping. Similarly, the self-blame dimension of coping had contributed to 10% variance in developmental burden, 22% variance in physical burden, and 5% variance in social burden dimensions of caregiver burden.
From Table 4, it is evident that the dimensions of spirituality contributed to significant proportion of variance in the dimensions of caregiver burden, making spirituality a major predictor of caregiver burden. The self-discovery dimension of spirituality had contributed to 4% variance in developmental burden and physical burden, 28% variance in emotional burden, and 7% variance in social burden.

The relationships dimension of spirituality also had made significant contributions in predicting caregiver burden. Relationships dimension had contributed to 6% variance in developmental burden, 6% variance in physical burden, 26% of variance in emotional burden, and 17% variance in social burden dimensions of caregiver burden.
The eco-awareness dimension of spirituality contributed to 4% variance in developmental burden, 34% variance in emotional burden, and 5% variance in social burden. Table 4 also showed that spirituality, as a whole had contributed to 8% variance in overall caregiver burden.
Furthermore, it can be observed from the Table 4 that none of the dimensions of spirituality have contributed to the time-dependency dimension of caregiver burden, indicating that time-dependency dimension of caregiver burden cannot be predicted by the dimensions of spirituality.
DISCUSSION
The analysis of the results of this study indicated that both groups of caregivers (mothers and fathers) had a similar experience of burden while caring for their child. Parents experience severe psychological distress when their child is diagnosed with a serious illness like ALL. Gender roles may have an impact on who is providing physical or emotional caregiving, but the diagnosis, the treatment process and the prognosis of the disease are equally challenging for both the parents.[21]
Men and women differ to a greater degree in their expression of emotions, perception of the situation, and coping styles.[22] The results of the current study are concurrent with the available literature revealing the differences in the coping strategies availed by mothers and fathers. Mothers used religion, emotional, and instrumental support more than the fathers whereas, fathers used substance intake and acceptance of the situation more than the mothers. Religiosity or use of religion has been consistent with the conventional literature which suggests that women are more likely to express greater interest in religion and are thus more religious when compared to men. The reason why women tend to have stronger religious commitment than men could be attributed to differential socialization that encourages women to possess traits that are highly associated with religiosities such as nurturance and obedience and these traits have been proven to be greater predictors of religiosity.[23] Possessing such personal commitment and interest in religious beliefs and values encourages women to therefore use it as a coping strategy to deal with stressful life events. Women also tend to be more inclined to the use of emotional support as a means to cope with life stressors. Even in this scenario, conventional beliefs hold that women are more emotional and emotionally expressive than men [24] and similar to religiosity, emotional expressiveness has only been linked to socialization, wherein early instillation of socially acceptable display of emotions in women lead to their emotional expressivity, and thus, women are highly emotionally expressive than men.[25] Thus, femininity was associated with receiving and seeking emotional support and that too from women.[26] A study on male caregivers revealed that male caregivers are more inclined to use informal support [27] when compared to their gender counterparts.[2829] A study on use of social support and gender differences showed that although men tend to receive social support, it was only limited to receiving tangible or instrumental support.[26] Having stated this, the results of the current study showed that, women, along with emotional support, are high on using instrumental support as well when compared to men. The argument could be that, social support is a broader term that largely encompasses several domains such as emotional support, instrumental/tangible support, intangible support, informational support, and even religious support, and women seemed to be high on seeking out for and receiving social support overall, whereas men availed a particular domain of social support that is the instrumental or tangible support.
Apart from these, the results of the current study showed that male caregivers (fathers) were high on using substance as a means of coping. A study conducted on alcohol and stress showed that existence of stressors highly predicted both alcohol use and drinking problems among men, especially in those men who held strong positive expectations from the effects of alcohol. This also held true for those men who used avoidant forms of emotion coping.[30]
The current study also identified that those mothers were found to be higher on eco-awareness subscale of spirituality. No significant difference was observed between mothers and fathers on the other two subscales of spirituality, namely, self-discovery and relationships. There has been no empirical data available to examine the differences between men and women on their levels of spirituality, but the difference between the two groups in this particular dimension (eco-awareness) could probably be attributed to the connection that women tend to have with the environment or nature that could be viewed through the “ecofeminism paradigm” which looks at sexism or patriarchy as parallel to exploitation of the environment and that both these are considered as “forms of domination,” the former being domination against women and the latter against the environment.[31] Furthermore, not much research has been done in the field of eco-awareness concept of spirituality.
Coping mitigates the stress that the caregivers experience.[32] In the present study, positive reframing predicted all five dimensions of caregiver burden. Acceptance was also found to be negatively correlated with physical burden, and social burden, stating that physical and social functioning of caregivers can improve when they accept the condition of their child. Self-distraction, behavioral disengagement, use of emotional support, instrumental support, and religion were found to be significant modifiers of caregiver burden.
Spirituality was a significant predictor of emotional, physical, developmental, and social burden. The relationships dimension of spirituality predicted four dimensions of caregiver burden, indicating that maintaining and valuing relationships had an effect on their caregiver stress, probably because relationships provide emotional support and tangible support at the time of crisis. Spirituality buffered the adverse effects of stress and incorporating the spiritual component into coping styles may help in developing effective coping interventions.[33] The ability to develop and implement effective coping strategies, (tailored according to the individual needs) is of utmost importance during a crisis, as it mitigates the intensity of caregiver burden.
Spirituality, in the present study, was seen to decrease the experienced burden of the caregivers and improve their well-being. A multidimensional construct such as spirituality could serve as a reliable resource for coping and improving the overall well-being of caregivers. Identifying the existence of spiritual factors and coping styles and their role in improving the quality of life among caregivers is vital to develop effective coping strategies to match individual needs.
CONCLUSION
Parents experience as caregivers is extremely stressful and challenging. While caregivers manage to deal with their distress, it is important that they receive professional help in handling their physical and emotional distress. The current study has its implications in planning and designing effective interventions, to relieve caregivers of their burden. Effective coping strategies can help caregivers provide the best support to their sick child, at the same time handle their own distress developing effective strategies. Incorporating the spiritual component while designing an intervention will mitigate caregiver burden, enhance physical and psychological wellbeing and equip them adopt the caregivers role. It is essential that the hospital authorities and policymakers understand that a professional health psychologist could be a liaison between the doctor, patient, and the caregiver in bringing down the levels of burden and psychological distress in caregivers as well as patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 2012. American Cancer Society, Cancer Facts & Figures. Available from: https://www.cancer.org/cancer/cancer-in-children/key-statistics.html
- Acute leukemia in children: A review of the current Indian data. South Asian J Cancer. 2016;5:155-60.
- [Google Scholar]
- Family caregiver burden: Results of a longitudinal study of breast cancer patients and their principal caregivers. CMAJ. 2004;170:1795-801.
- [Google Scholar]
- Psychosocial study of leukemic children and their parents. Indian Pediatr. 1992;29:985-90.
- [Google Scholar]
- Coping and adaptation in parents of children suffering from acute lymphoblastic leukemia. Indian J Pediatr. 1995;62:737-41.
- [Google Scholar]
- Burden and coping of caregivers of physical and mental illnesses. Delhi Psychiatry J. 2013;16:367-74.
- [Google Scholar]
- A Study of Stress and Coping Strategies of Caregivers of the Demented Elderly. Hong Kong University Dissertation; 1998. p. :1-0.
- Coping among the caregivers of patients with schizophrenia. Ind Psychiatry J. 2015;24:5-11.
- [Google Scholar]
- Burden and coping strategies in caregivers of stroke survivors. J Neurol Neurosci. 2015;1:1-5.
- [Google Scholar]
- Body, mind and spirit: Towards the integration of religiosity and spirituality in cancer quality of life research. Psychooncology. 1999;8:439-50.
- [Google Scholar]
- The role of religion/spirituality for cancer patients and their caregivers. South Med J. 2004;97:1210-4.
- [Google Scholar]
- The role of religion/spirituality in coping with caregiving for disabled elders. Gerontologist. 1998;38:463-70.
- [Google Scholar]
- The effect of spirituality and gender on the quality of life of spousal caregivers of cancer survivors. Ann Behav Med. 2007;33:90-8.
- [Google Scholar]
- Religiosity and perceived rewards of black and white caregivers. Gerontologist. 1997;37:89-101.
- [Google Scholar]
- The emotional impact of caring for the chronically ill. Psychosomatics. 1990;31:331-6.
- [Google Scholar]
- New Study Identifies Challenges for Family Caregivers, Caregiving Solu; 04 June, 2015. Available from: http://wwwprwebcom/releases/2015/06/prweb12765231.htm
- Psycho-oncology research in India: Current status and future directions. J Indian Acad Appl Psychol. 2008;34:7-18.
- [Google Scholar]
- You want to measure coping but your protocol's too long: Consider the brief COPE. Int J Behav Med. 1997;4:92-100.
- [Google Scholar]
- The spirituality scale: Development and psychometric testing of a holistic instrument to assess the human spiritual dimension. J Holist Nurs. 2005;23:145-67.
- [Google Scholar]
- Application of a multidimensional caregiver burden inventory. Gerontologist. 1989;29:798-803.
- [Google Scholar]
- The challenge of quality care for family caregivers in pediatric cancer care. Semin Oncol Nurs. 2012;28:213-20.
- [Google Scholar]
- Risk and religion: An explanation of gender differences in religiosity. J Sci Study Relig. 1995;34:63-75.
- [Google Scholar]
- Sex differences in emotion: Expression, experience, and physiology. J Pers Soc Psychol. 1998;74:686-703.
- [Google Scholar]
- Gender and emotional expressiveness: An analysis of prosodic features in emotional expression. Pragmat Intercult Commun. 2012;5:46-54.
- [Google Scholar]
- Use of social support: Gender and personality differences. Sex Roles. 2001;44:437-59.
- [Google Scholar]
- Gender differences in psychiatric morbidity among family caregivers: A review and analysis. Gerontologist. 2000;40:147-64.
- [Google Scholar]
- Males as helpers: The role of sons, relatives, and friends. Gerontologist. 1990;30:228-35.
- [Google Scholar]
- Gender differences in caregiver stressors, social resources, and health: An updated meta-analysis. J Gerontol B Psychol Sci Soc Sci. 2006;61:P33-45.
- [Google Scholar]
- Stress and alcohol use: Moderating effects of gender, coping, and alcohol expectancies. J Abnorm Psychol. 1992;101:139-52.
- [Google Scholar]
- Warren KJ, ed. Ecological Feminism. New Work: Routledge; 1994.
- Coping and depression in Alzheimer's caregivers: Longitudinal evidence of stability. J Gerontol B Psychol Sci Soc Sci. 2002;57:P205-11.
- [Google Scholar]
- Spirituality moderates the effect of stress on emotional and physical adjustment. Pers Individ Dif. 2002;32:1377-90.
- [Google Scholar]




