
Translate this page into:
Does Pain Behavior Influence Assessment of Pain Severity?
Address for correspondence: Dr. Geetha Desai; E-mail: desaigeetha@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Nurses are involved in assessment of pain in most clinical settings. Pain continues to be underestimated and undertreated.
Materials and Methods:
This study assessed the rating of pain severity by nurses who observed the two case scenarios using role plays. The data were computed and frequency distribution was derived.
Results:
Majority of the nurses underrated the pain and based their ratings on various factors.
Conclusions:
It is important to increase the awareness among nurses about comprehensive assessment of pain for better management.
Keywords
Pain assessment
Pain behaviors
Pain severity

INTRODUCTION
A lack of comprehensive assessment of pain can lead to poor management or treatment of pain. Nurses are often involved in the assessment of pain. Pain, defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage (IASP)[1], is a subjective experience and this is taken into account while assessing the intensity of pain.
A study conducted in a Saudi hospital assessed the opinion of nurses on self report of pain as the indicator of pain intensity revealed that nurses underestimated pain intensity in smiling patient and overestimated it in the grimacing patient (Kaki et al. 2009).[2]
McCaffery et al. (2000)[3] conducted a survey of nurses' decisions about assessment and treatment of pain in two patient situations and confirmed that nurses continue to under treat severe pain. As shown in previous studies, nurses may be more influenced by the patient's behavior than the patient's self-report of pain. Surveys have shown that patient self-report of pain is often not considered as a reliable indicator of pain (Pederson 1997, Sloman et al. 2005, Zalon 1993)[456].
In a recent report, Desai, Chaturvedi (2009)[7] reported that majority of the nurses considered pain behaviors and ignored the subjective component of pain when they were asked to rate the pain on two case vignettes.
This study analyses nurses rating of intensity of pain after assessing two mock clinical situations using role plays.
MATERIALS AND METHODS
The sample was formed by the participants of series of workshop on chronic pain that are being conducted for the health professionals. A workshop was conducted for the postgraduate nursing students at National Institute of Mental Health and Neuroscience, Bangalore India in November 2009. Two role plays were done by the participants on assessment of pain when the other participants were asked to assess the severity of pain. The instructions for the participants doing role play were explained during the workshop. The case scenarios are given below. The participants were asked to observe the interview and rate the severity of pain and suffering on a visual analogue scale (VAS) of 0-10 in both the cases. They also were asked to cite the reasons for their rating. The vignettes and the questions are given below. The participants provided written informed consent for participation in this exercise.
A 35-year-old woman has been admitted with history of pain in lower back since 1 year. You are asked to assess the severity of pain and rate the pain on VAS. Her vitals are stable.
You are a 35-year-old woman who has been suffering from pain in her lower back since 1 year. You have been having very severe pain at times. On the day of your assessment your pain is severe and you are unable to sit comfortably, moaning in pain, holding your back with your hands. You are tearful when details about your pain are being asked. You rate your pain as 7 on the VAS, when asked.
A 39-year-old man has come with history of pain the upper back since 1 year. You are asked to assess the severity of pain and rate the pain on VAS. On examination vitals are stable.
You are a 39-year-old man who has been suffering from pain in his upper back since 1 year. You have been having very severe pain at times. On the day of your assessment your pain is severe and you are unable to sit comfortably. You are not showing signs of distress and trying to distract yourself from pain. You rate your pain as 7 on the VAS.
How would you rate their pain?
You need to document their pain in their charts using 0-10 scale. Put 1 next to the rating you would record for Case 1 and 2 next to the rating you would record for Case 2 pain.
0---------1---------2--------3------4------5------6------7-------8------9-------10
Give reasons for your rating:
Case 1
Case 2
How would you rate the suffering for Case 1 and 2?
Put 1 next to the rating you would record for Case 1 and 2 next to the rating you would record for Case 2.
0---------1---------2--------3------4------5------6------7-------8------9-------10
Give reasons for your rating:
Case 1
Case 2
RESULTS
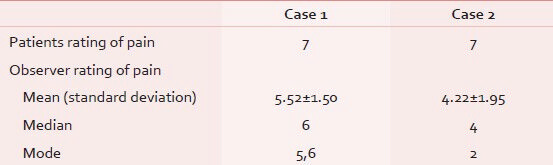
The total number of participants were 23. The sample consisted of 14 (61%) women and 9 (39%) men. In case scenario 1, only 4 (17%) participants rated the correct reported intensity of pain as 7. In case scenario 2 also, four (17%) rated the intensity of pain as 7. Three participants overrated the pain in both case scenarios. In both situations the pain was underrated, more so in the case scenario 2. In case scenario 1: only 2 (8.6%) participants received a score 2-3, 15 (65.2%) received a rating of 4-6. In case scenario 2: 10 (43.5%) participants received a score 2-3, 8 (34.7%) received a rating of 4-6. The mean, median, and mode for the above cases are shown in Table 1. In both the cases, the mean rating has been rated below 7, which is the expected rating.
The mean for suffering for the above cases were 5.48 ± 1.53 for Case 1 and 4.30 ± 2.12 for Case 2. In both cases the mean rating for suffering is below 7 which is the expected rating.
The reasons for rating pain intensity in case scenario 1:
-
Patient showed grimacing
-
Appeared uncomfortable
-
Cause was clear
The reasons for rating of pain in clinical scenario 2:
-
Functioning was not much affected
-
The patient was not using analgesics on daily basis
-
The patient did not show discomfort
-
The patient did not express pain and feelings
DISCUSSION
The findings illustrate that self report of pain is often not relied for rating the pain intensity by professionals. Nurses relied on their observation of the patient's behavior rather than on the self-report. The observed factors which they took into consideration for rating were facial expression, discomfort in maintaining posture during interview, interference with daily activities, use of analgesics and the cause of the pain. This study corroborates the findings of studies done in other clinical settings (McCaffrey et al. 2000, Kaki et al. 2009, Pederson et al. 1997.[324] The mean, mode, and median scores were lower for Case 2 who was not showing signs of distress and was trying to distract from pain.
Despite pain being highly subjective experience, the self-report is not taken into account as indication of pain intensity. A recent report used the written case scenarios methods and concluded that overt behavior and emotions determined pain ratings (Desai, Chaturvedi 2009),[7] and this report using clinical interview by role play method confirms that pain ratings are based on many factors and not actually by self report. This exercise was done as a part of microteaching, hence role play was used and the observers were asked to do the assessment of severity of pain along with assessment of other aspects of pain. This method for assessing observer bias in pain assessment has been reported in literature (Desai, Chaturvedi 2009, McCaffrey et al. 2000, Kaki et al. 2009, Pederson et al. 1997)[7324] as a reasonable method.
The above findings highlight the need for increasing awareness among nurses regarding assessment of pain. Health professionals and nurses should not get misled by overt behaviors and emotional distress expressed or suppressed, while assessing pain intensity, and should give credence to the subjective rating mentioned by the person in pain. A comprehensive assessment will lead to better management of pain.
Gender bias in assessment of pain is a possibility that has been raised. In order to maintain anonymity of the responses the participants were asked not to mention their personal details including gender. This is to have an authentic and reliable response by the participants. However, this could be a potential area for future research.
It is also important to study other factors which may influence the nurses' assessment of pain. A Manual of Chronic Pain assessment and management describes various methods for pain measurements (Chaturvedi, Desai 2009).[8][for a copy of the manual, please contact the author]
CONCLUSIONS
The study highlights that the overt behaviors of pain are given more precedence than the subjective report of the patient in assessment of pain by the nurses, which is misleading. A comprehensive pain assessment is more desirable and is likely to be accurate measure of pain. Since nurses play an important role in pain assessment and management it is important to increase the awareness among them by various educational methods. Factors which may confound pain assessment should be considered when doing pain measurement.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Part 3: Pain Terms, A Current List with Definitions and Notes on Usage. In: Merskey H, Bogduk N, eds. IASP Task Force on Taxonomy. Seattle: IASP Press; 1994. p. :209-14.
- [Google Scholar]
- Nurses' knowledge of pharmacological measures on acute pain management in western Saudi Arabia. Saudi Med J. 2009;30:279-83.
- [Google Scholar]
- Nurses' personal opinions about patients' pain and their effect on recorded assessments and titration of opioid doses. Pain Manag Nurs. 2000;1:79-87.
- [Google Scholar]
- Bone marrow transplant nurses' knowledge, beliefs, and attitudes regarding pain management. Oncol Nurs Forum. 1997;24:1563-71.
- [Google Scholar]
- Pain behaviours determine pain severity rating by nurses. Indian J pain. 2009;23:318-9.
- [Google Scholar]
- Assessment and management of chronic pain-a manual for pain clinicians. Bangalore: NIMHANS; 2009.




