
Translate this page into:
Effect of Nation-wide Lockdown on Palliative Care Services in a Tertiary Care Centre in India: A Retrospective Observational Study
Address for correspondence: Prof. Sushma Bhatnagar, Department of Onco-Anaesthesia and Palliative Medicine, DR. BR Ambedkar Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi - 110 029, India. E-mail: sushmabhatnagar1@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
The ongoing coronavirus disease 2019 (COVID-19) pandemic has affected all the aspects of life of mankind, posing unique challenges for health-care services. In order to contain the spread of the virus, a countrywide mass lockdown has been imposed in India. Although the lockdown has modified the epidemic trajectory, it has affected the lives of many non-COVID patients. Patients in need of care could not approach hospitals.
Methods:
This retrospective observational study was conducted in the Department of Onco-Anaesthesia and Palliative Medicine at a tertiary care center in India. The yearly data of patient flow for the year 2019 was compared with that during the lockdown.
Results:
The single-day average of out-patients, in-patients, and other department consultation requests requiring palliative care decreased drastically during the lockdown in comparison to the previous year. The single-day average of teleconsultations increased more than double during the lockdown.
Conclusion:
Although lockdown decreases the spread of the epidemic, it increases the suffering of other patients who require medical care. Various steps have to be adopted in the regular working pattern of hospitals to cater to the needs of the patients requiring care, without increasing the risk of contracting COVID-19.
Keywords
Coronavirus disease
lockdown
palliative care

INTRODUCTION
The ongoing coronavirus disease 2019 (COVID-19) pandemic which originated in Wuhan, China, in December 2019 has produced multifold repercussions on all the aspects of life of mankind on this planet. Health-care services have been posed with unique challenges worldwide. In countries such as Italy and Spain, healthcare facilities have been overwhelmed during the peak of the outbreak. The total number of cases crossed over 44 lakhs worldwide, with over 2.9 lakh deaths and 16 lakhs being recovered as on May 13, 2020.[1] In India, the number of cases has been on an increasing trend since the first case was reported in the late January 2020. The nation has been under lockdown in an attempt to contain the spread of the virus since March 25, 2020, for over 50 days when this article was written. The total number of cases in India crossed over 78,000 as on May 13, 2020, with over 2500 deaths.[1] The number of cases has been on an increasing trend and with the extrapolation of data it seems that the virus will stay with us for some more time. In the absence of any established treatment or vaccine till now, various public health measures such as travel restrictions, mass lock down, advisory on mass gatherings, and public health events have been issued by the government to modify the epidemic trajectory.[23] These measures aim to prevent the growth of cases as well as reduce the number of cases, meanwhile providing opportunities for strengthening our health system to face the upcoming surge of cases once lockdown is lifted upon.
Apart from the effect on the growth of cases, lockdown has influenced various other aspects of routine life. It has produced significant changes in the dynamics of patient flow among hospitals in India. While preparing health services for COVID cases, many of the non-COVID patients are suffering due to interruption in their treatment, be it curative or palliative. This may increase the suffering and also affect their quality of life. Palliative care is the active holistic care of individuals across all ages with serious health-related suffering due to severe illness and especially of those near the end of life. It aims to improve the quality of life of patients, their families, and caregivers.[4] In India, the provision of palliative care services is limited to tertiary care institutes in most of the regions except Kerala. Lockdown has prevented the patients in need to reach out to these places for care. This retrospective observational study was done to assess the effect of the nation-wide lockdown on the patient flow dynamics in the department.
METHODS
This retrospective observational study was conducted at the Department of Onco-Anaesthesia and Palliative Medicine at a tertiary care center in India. The department caters to the palliative care needs of cancer and noncancer patients through inpatient, outpatient, and on-call services. The yearly data of patient flow for the year 2019 was compared with the data during the first 50 days of the nationwide lockdown from March 25, 2020, to May 13, 2020. The data for outpatient services (new registrations and follow-up visits), inpatient services (number of admissions), telemedicine services (number of calls), and oncall services (consultation requests from other departments) were studied.
RESULTS
A total of 1219 new registrations and 16,448 follow-up visits were done in the Pain and Palliative Care Out-Patient Clinic during the year 2019 [Figure 1]. During the first 50 days of the lockdown, 25 new registrations and 797 follow-up visits were seen in the clinic. A total of 1474 admissions were done in the palliative care unit in 2019 [Figure 2]. The number of inpatient admissions done during the lockdown period was 22 out of which 6 were during the first 30 days of lockdown and 16 were during the next 20 days. The major indications for admission were analgesic titration for acute exacerbation or severe chronic cancer pain, therapeutic pleurocentesis and peritoneocentesis, management of sub-acute intestinal obstruction, malignant spinal cord compression syndrome, and interventional pain blocks. A total of 826 consultation requests from other departments were attended in 2019 [Figure 3]. During the lockdown, 94 consultations were attended. These included calls for symptom management, including cancer pain, noncancer pain and oral mucositis, management of dyspnea, palliative intervention procedures, counseling about the prognosis, and end of life care. About 985 telephone calls from patients were answered during the year 2019. The number of telephone consults received was 314 during the lockdown. The single-day average of all of the above data is shown in [Figure 4] for comparative analysis.
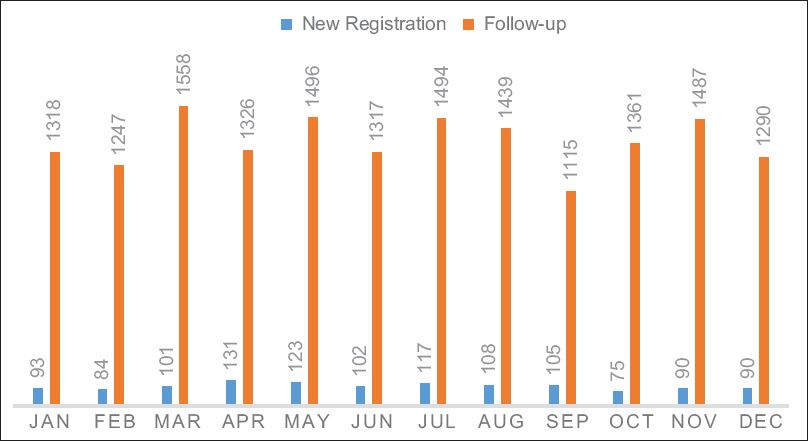
- Outpatient services for 2019
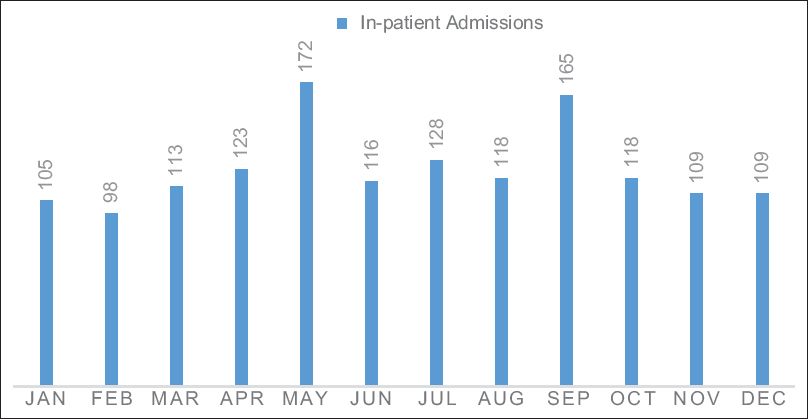
- In-patient admissions for 2019
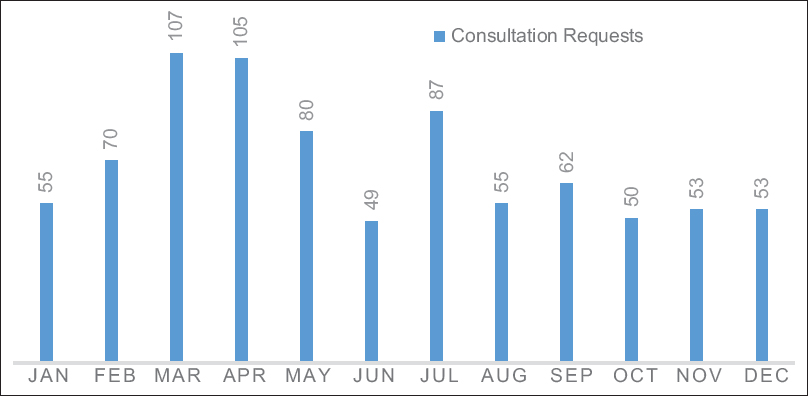
- In-hospital consultation requests in 2019
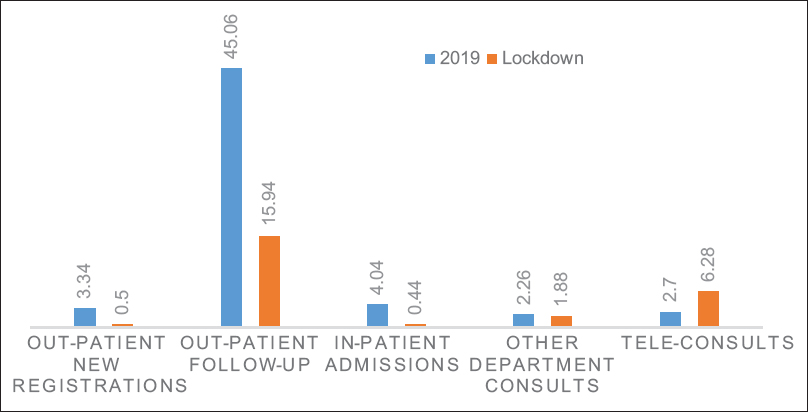
- Single day average of patient flow data
DISCUSSION
The number of outpatients dropped by a huge margin during the lockdown mainly due to the interstate and intrastate travel restrictions and governmental advisory of avoiding visits to the hospitals for nonurgent reasons. To reduce the hospital visits of the patients and reduce the crowd in hospital, we had changed the departmental protocol and issued medications (including opioids) for 1 month instead of the usual protocol of 2 weeks. The patients who were not on opioids were encouraged to get the medicines from nearby pharmacies after teleconsultation. In the absence of fresh complaints, they were discouraged to visit the hospital during lockdown just for the sake of getting medicines. Those patients who received opioids were asked to visit either our hospital or any hospital in their vicinity when their medications finished.
The inpatient admissions drastically reduced, especially during the early days of the lockdown. This was due to the overall reduction in patient inflow to the hospital. Those patients who consulted telephonically and seemed to require inpatient care were unable to approach the hospital or did not wish to visit the hospital. They were asked to visit nearby hospitals and necessary advice was given telephonically. Hence, the overall admissions had decreased. During the latter days of lockdown, when restrictions were eased, in-patient admissions increased to a small extent. We had converted our six bedded palliative care unit to a four bedded unit to ensure safe distancing between beds. This will continue to be an important reason for reduced admission of patients even when the lockdown is lifted. All the patients were screened for any symptoms suggestive of COVID before admission. If any patient was suspected to be a COVID case, then the Department of Infectious Diseases was involved to proceed for testing, contact tracing, and planning further course of action. Patients were educated regarding the Do's and Don'ts during their hospital visit, cough etiquette, hand hygiene and were urged to practice social distancing during their hospital stay. Patients and their attendants were advised to wear a mask always and only one attendant could stay with the patient, to reduce the risk of cross infection. Instead of gathering at a single place, patients were asked to wait patiently in a queue. The hospital administration actively arranged for personal protective equipment for all the health-care workers that boosted the confidence of all health-care professionals to practise their clinical duties toward the patients.
Consultation requests from other departments reduced due to the overall reduction in bed occupancy of all wards in the hospital. The number of teleconsultations more than doubled during the lockdown. There were many reasons for this rise. Earlier the department had only a basic feature phone for teleconsultations. Just before the lockdown, anticipating the necessity, the department procured a dedicated smartphone for teleconsultation services. The smartphone was internet enabled and WhatsApp™ messaging service was initiated. This allowed multimedia communication with the patients. The service was available round the clock. Patients visiting the outpatient service were encouraged to use this new service. Those patients who did not visit the hospital during the lockdown and called us on the old number were informed of the new development and encouraged to utilize the new service. The media outreach and computer facility of the hospital reached out to patients and created the awareness about the improved teleconsultation services. All of these measures cumulatively enabled us to provide safe patient care even during one of the longest lockdowns of the country.
Another point to be highlighted is that despite all our efforts, though we could cater many of the patients, one cannot overlook the importance of decentralization of palliative care services to primary health care level from tertiary care centers and provisions for availability of opioids in peripheral centers. One cannot ignore that the basic health services at primary level needs major reforms so that we can reach out to our population. This pandemic has once again highlighted the importance of reforms in the health-care sector in India.
CONCLUSION
Health-care delivery is not going to be the same what it used to be a few months earlier. With the ongoing developments, it seems that COVID-19 is going to stay for some more time. Lockdowns help in reducing the spread of the disease. However, it creates a considerable amount of burden among non-COVID patients. Patients requiring palliative care cannot be asked to indefinitely postpone their interaction with palliative care physicians. Doing so would demolish the basic essence of palliative care - reducing suffering.[4] Patients receiving opioids should be able to get their medicines replenished in time to avoid withdrawal effects and reappearance of symptoms. Hence, palliative care units should adopt new strategies and innovations in their delivery of services until this pandemic comes to an end.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Available from: https://wwwworldometersinfo/coronavirus/
- Available from: https://pibgovin/PressReleseDetailaspxPRID=1614255
- Available from: https://pibgovin/newsite/PrintReleaseaspxrelid=200655
- Redefining Palliative Care – A new consensus-based definition. J Pain Symptom Manage 2020 May 6 S0885-3924(20)30247-5 doi: https://doiorg/101016/jjpainsymman202004027 Online ahead of print
- [Google Scholar]




