
Translate this page into:
Nonpharmacological Interventions for Pain Management in Lung Cancer Patients: A Systematic Review
Address for correspondence: Dr. Jayaprakash Kumar, Department of Preventive Medicine, University of Tennessee Health Science Center, 66 N Pauline St., Memphis, TN 38163, USA. E-mail: jkumar7@uthsc.edu
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
The presence of lung cancer is almost always associated with pain, a symptom that causes severe distress in patients. Although many pharmacological methods are available to manage pain in this oncologic population, the medications often cause undesirable sideeffects and inadequate relief. Nonpharmacological interventions can be used as adjuvants to pharmacological interventions in reducing pain and increasing quality of life.
Objectives:
The purpose of this review is to compare the efficacy of nonpharmacological interventions in reducing pain in lung cancer patients.
Materials and Methods:
This is a systematic review study guided by the Preferred Reporting Items of Systematic reviews and Meta-Analysis Protocol. Interventions identified in the present systematic review have been categorized as physical treatment, technologybased, cognitive behavioral, coping, and coaching.
Results:
Results indicate that the nonpharmacological interventions such as physical treatment interventions, selfmanagement and coaching interventions, cognitive behavioral interventions, and technologybased interventions or coping skills interventions had limited and shortterm effects on alleviating pain among the patients. However, previous studies have provided limited evidence regarding nonpharmacologic therapy due to the lack of a comparison group, small sample sizes, and lack of longterm followup periods to determine whether sustained effects are feasible.
Conclusion:
Healthcare professionals should consider additional research on the added advantage of utilizing the nonpharmacological interventions as an adjunct option while managing pain in lung cancer patients.
Keywords
Lung cancer
nonpharmacological
pain management

INTRODUCTION
Lung cancer is the leading cause of death among all types of cancers in the US.[1] New cases of lung cancer in 2016 are estimated to be 13% of all cancers, only second to breast cancer in women and prostate cancer in men.[1] Lung cancer patients report a myriad of physical and psychosocial symptoms varying from pain, fatigue, dyspnea, and coughing to distress, anxiety, and depression.[2] Pain remains one of the most distressful symptoms in cancer patients[3] which affects patients' quality of life and psychosocial functioning.[4567] Manifestation of lung cancer pain is multi-faceted due to tumor location, spread of tumors, stage of metastases, existence of other comorbidities, and anti-cancer treatment.[78]
Evidence-based pharmacological interventions indicate that the use of opioid analgesics and surgical interventions are the most common lung cancer pain management methods.[8] However, pharmaceutical pain management methods, especially opioid analgesics often have unreliable pain control and frequently cause adverse effects.[910] To overcome these limitations, nonpharmacological approaches including prophylactic and complementary interventions[1112] have been suggested to alleviate pain. A systematic review on nonpharmacological interventions of pain management in cancer patients in general conducted between 2010 and 2013[13] concluded that the effectiveness of those interventions was rather limited with only a short-term effect. To our knowledge, there is no evidence of a systematic review that focuses on the efficacy of nonpharmaceutical pain management interventions conducted among only lung cancer patients. As such, we aim to build on the prior knowledge and systematically review the various nonpharmacological interventions for pain in lung cancer patients over the past 5 years.
METHODS
Study design
Methods and presentation of results for this systematic review were guided by the Preferred Reporting Items of Systematic Reviews and Meta-Analyses Protocol.[14]
Literature search
The literature search involved a systematic search of five journal indexing databases: CINAHL, PubMed, PsycInfo, Scopus, and Web of Science. Each database was searched for relevant articles using the key terms (lung cancer OR lung neoplasms OR thoracic cancer) AND Pain AND (intervention OR program OR management) AND (nonpharmacological). In addition, cross-referencing the articles was performed.
Inclusion/exclusion criteria
Studies were included in this systematic review if interventions were published in English and evaluated the symptom of pain in lung cancer patients (any type and any stage) between January 2010 and December 2015. Interventions that had <five patients per treatment arm were excluded from the study.
Study selection
Two reviewers independently performed the search selection and numbers of references were compared at each step of data extractions. If difference in the numbers were found, the two reviewers discussed the reasons for discrepancies and reached a consensus.
Data extraction
Relevant references were pooled into a database and were reviewed for relevance after elimination of duplicates. Reviewers identified relevant studies and extracted the following information: Authors, year of study, geographic location of study, study design, sample and population setting, measurement tools for outcome, intervention used, and statistical inferences [Table 1]. The overall quality of the methodology of the systematic review was assessed by the assessment multiple systematic reviews[15] criteria and quality of individual interventions with a 27-item quality assessment checklist.[16] Nonrandomized trials scores varied from 23 to 27 and randomized controlled trials' (RCT) scores were in the range of 22–27, indicating the quality of the interventions where a score of 26–28 = excellent; 20–25 = good; 15–19 = fair; and ≤14 = poor.[16]
| Author/Year | Population setting | Aim/purpose of the study | Study Design/ Intervention | Examination/Outcome measure | Findings/Results |
|---|---|---|---|---|---|
| Cheville et al, 2013, USA Home-based exercise intervention | 60 adults; 35 Males, 25 Females; Stage IV lung or colorectal cancer. | To conduct an adequately powered trial of a home-based exercise intervention | Initial one-on-one, 90-minute instructional session in Rapid, Easy, Strength Training (REST) as well as a pedometer based walking program | Numeric Rating Scale for pain (NRS) | Control group: Mean difference -0.50 On NRS (SD 2.01, 95% CI, -1.25, 0.25) Intervention group: Mean difference -0.62 (SD 2.59, 95% CI, -1.66, 0.43) No significant difference in the pain scores-(p Value-0.87) |
| Gale et al, 2012, UK Choral singing |
30 adults (patients & caregivers); 23 Males, 7 Females; Mean age 60 yrs) Lung cancer |
To examine changes in Quality of Life (QOL) and fatigue following the participation in a choir using a mixed methodological approach in subjects who have received treatment for cancer and their families | Choral singing, Individuals regardless of musical experience or ability, with weekly rehearsals for a minimum of 2 hours | RAND 36-Item Short Form Health Survey questionnaire |
Pre-Choir: RAND 62.1 (28.8) 3 Months Post-Choir: RAND 72.9 (28.2) Improved bodily pain (p-value 0.010) |
| Koller et al, 2013, Germany Self-management (information provision, skills building, and nurse coaching) |
39 adults; 20 Males, 19 Females; Oncology outpatients from a Comprehensive Cancer Left in Freiburg, Germany lung, breast, renal, prostate, colon, oropharynx, pleura, and pancreas | To evaluate and demonstrate the feasibility of a U.S.-developed cancer pain self-management intervention | The intervention employed three strategies: information provision, skills building, and nurse coaching. | Changes in average and worst pain intensity | Average and worst pain scores did not Demonstrate any statistically significant group-by-time interaction effects between the intervention and the control group, either over the 10-week intervention period (p ¼ 0.48/p ¼ 0.60) or over the 22- week study period (p ¼ 0.89/p ¼ 0.90). |
| Kwekkeboom et al, 2010, USA Cognitive behavioral intervention (e.g., relaxation, guided imagery, nature sound recording) | 30 adults; 6 Males, 24 Females; advanced metastatic or recurrent) colorectal, lung (27%), prostate, or GYN cancers; 36-79 Yrs,Caucasian 26 (87) African American 2 (7) Missing 2 (7), Comprehensive Cancer Center in the Midwestern United States. | To evaluate the feasibility of a patient-controlled cognitive behavioral intervention for pain and other symptoms. | Training to use an MP3 player loaded with 12 cognitive-behavioral strategies | Numeric rating scale (NRS), Brief Pain Inventory (BPI) | Average pain scores on NRS decreased from M=4.54 (SD=2.27) pre-treatment to M=2.77 (SD=2.06) post-treatment (Z=−4.20, p <.01). Immediate changes in pain ratings from pre- to posttest treatment were significant P < 0.01. |
| Lopez et al, 2012, USA Physiotherapy intervention (massage & exercise) Oncology University Hospital Salamanca | 24 patients (18 males, 6 females) with terminal cancer (diagnosed with any type of tumor in stage III-IV,) lung, melanoma, sarcoma, pancreas, breast | To determine the effects of physical therapy, including massage and exercise, on pain and mood in patients with advanced terminal cancer | Physiotherapy Intervention consisting of several massage techniques, mobilizations, and local and global exercises. OR simple hand contact/touch to areas of pain | Brief Pain Inventory (BPI), Memorial Pain Assessment Card (MPAS) | Improvements in the intervention group were significantly greater than in the control group for the first evaluation (worst pain and current pain) and for the first and second evaluation (total BPI index). By contrast, the comparisons did not reveal significant differences for BPI pain on mean (F=2.160, P=0.127) and least pain (F=0.576, P=0.027) |
| Somers et al, 2015, USA Coping skills training (e.g., Internet pain coping skills sessions) | 25 patients with cancer (17 males, 8 females) who had a diagnosis of breast, lung, colorectal, or prostate cancer, Duke University Medical Center | To examine the feasibility and acceptability of a brief PCST intervention delivered to patients in their homes using mobile health (mHealth) technology | Pain coping skills training (PCST) with m Health technology | Brief Pain Inventory, Chronic Pain Self-Efficacy Scale, Coping Strategies Questionnaire | There were no statistically significant changes in pain self-efficacy; however, the mean score on pain self-efficacy did increase (M =58.08, SD=17.17 vs. M=62.57, SD=13.82, t =1.34, P =0.19). |
| Wilkie et al, 2010, USA Sensory pain self-monitoring and coaching | 151 patients (108 males, 43 females) who had a diagnosis of small cell or non-small cell Lung cancer (Washington and Chicago area) | To examine effects of sensory self-monitoring and reporting Coaching on pain-related variables in patients with Lung cancer | sensory self-monitoring and reporting coaching | Pain Intensity Number (PIN) Scale, McGill-Pain Questionnaire (MPQ) | No significant statistical difference, but Coaching increased the amount of pain data communicated to providers by patients with Lung cancer, the magnitude was small |
| Kwekkeboom et al, 2012, USA Cognitive behavioral intervention (e.g., relaxation, guided imagery, nature sound recording) | 86 patients (35 males, 51 females) with advanced lung, prostate, colorectal, or gynecologic cancers receiving treatment at a National Cancer Institute-designated comprehensive cancer center in the midwestern U.S. | To assess initial efficacy of a patient-controlled cognitive-behavioral (CB) intervention for the pain, fatigue, and sleep disturbance symptom cluster | patient-controlled cognitive-behavioral (CB) intervention | Numeric Rating Scale (NRS) | Persons in the PC-CB intervention group re-ported less pain severity at Time 2 (MAdj =1.99, SE=0.30) compared with those in the control group (MAdj=3.23, SE=0.37), F=6.70, P=0.006 (effect size partial n2 =0.093, CI >0.021) |
| Schmidt et al, 2015, Germany Patient empowerment intervention (e.g., information booklet & diary keeping) | 652 patients (447 males, 205 females) at two tertiary medical care university hospitals (two tertiary medical centers) gastro-intestinal, genitourinary, gynecological or thoracic cancer | To explore the effect of patient empowerment on short- and long-term outcomes after major oncologic surgery in elderly cancer patients. | patient empowerment through information booklets which had information about surgery, anesthesia and perioperative management. A diary was maintained for a week to record pain and other significant events. | Health related quality of life (HRQoL) | Less pain in intervention group on 1st postoperative day (n=628) Intervention-234 (75.2%) No intervention- 261 (82.3%) p Value 0.03 |
| Rodriguez et al, 2010, USA Narrative therapy (individually tailored and multi-component intervention) | 72 subjects with non-metastatic breast, lung and colon cancer and depressive disorder (patients receiving ambulatory care at La Paz Hospital and Principe de Asturias Hospital (Madrid, Spain) | To compare narrative therapy (NT) plus escitalopram versus escitalopram plus usual care on quality of life and depressive symptomatology of depressed patients with oncologic disease. | Maybe pharmacological? | The Treatment of Cancer Quality of Life Questionnaire Core (EORTC QLQ-C30, version 1.0) | The combined therapy group showed significantly greater improvement in pain scale (p50.02) |
| Porter et al, 2011, USA Coping skills training intervention | 233 Lung cancer patients (52.8 % male patients, 31.0% caregiver males (from diagnosis of early stage Lung cancer (non-small-cell Lung cancer Stages I to III or limited-stage small-cell Lung cancer) and their caregivers | To determine the efficacy of a caregiver-assisted CST protocol in a sample of patients with Lung cancer. | Caregiver-assisted CST consisted of training in symptom management strategies. Sessions were supplemented with written materials A CD /audiotape with instructions for progressive muscle relaxation | Chronic Pain Self-Efficacy Scale (CPSES) | Patients in both treatment conditions showed improvements in pain significant main effects of time for ratings of worst pain (B =0.15, SE=0.13, P=0.02); |
| Henke et al, 2014, Germany Physiotherapy (strength & endurance training) | 46 patients, diagnosed with non-small cell Lung cancer (NSCLUNG CANCER) or small cell Lung cancer (SC LUNG CANCER) in stage IIIA/IIIB/IV, who received an inpatient palliative platinum-based chemotherapy treatment | To study the effects of a specially designed strength and endurance training on the independence and quality of life in Lung cancer patients | Strength and endurance training (four different endurance strength exercises were combined training trunk stability, leg, arm, and abdominal musculature. The functional endurance training consisted of two separate exercises, a walking exercise in the hallway and a stair walking exercise. | Treatment of Cancer Quality of Life Questionnaire Core-30 (EORTC QLQ C-30/LUNG CANCER-13) questionnaire | Improved pain outcome in the intervention group, pain in arms or shoulder, p =.048; |
| Lengacher et al, 2012. USA Mindfulness-based stress reduction intervention | 26 patient-caregiver dyads (patients were women and men aged 21 years or older diagnosed with Stage III or IV breast, colon,lung, or prostate cancer); had completed surgery; were undergoing treatment with radiation and/or chemotherapy) | To investigate whether a mindfulness-based stress reduction program for cancer improved symptoms, among advanced-stage cancer patients and caregivers. | Mindfulness-based stress reduction program (MBSR is a clinical program that provides systematic training to promote stress reduction by self-regulating arousal to stressful circumstances or symptoms) | The Medical Outcomes Studies Short-Form General Health Survey (MOS SF-36) | Improved outcomes of MOS SF-36. |
| Carlson et al, 2012, Canada Screening for distress symptoms intervention | 549 patients (300 males, 249 females, Mean age 63.5 yrs) with Lung cancer/problems attending a large tertiary cancer | To examine the impact of an online routine screening for distress program on physical symptoms and common psychosocial and practical problems in Lung cancer outpatients | Online routine screening for distress program | Continuous pain score(Pain thermometer)? | Patients reported few physical and psychological problems |
| Brocki et al, 2014, USA Exercise training (group training) | 78 patients undergoing Lung cancer surgery (42 males, 36 females Mean age 66.5 yrs) | To evaluate the short and long-term effects of supervised group exercise training on health-related quality of life and physical performance in patients, who were radically operated for Lung cancer | Supervised group exercise training | Health-related quality of life (HRQoL.) | Statistically significant effect after four months in the bodily pain domain of SF36, with an estimated mean difference (EMD) of 15.3 (95% CI: 4 to 26.6, p=0.01) |
| Van den Hurk et al, 2015, Netherlands Mindfulness-based stress reduction intervention | 19 patients diagnosed with cytological or histological proven non-small cell or small cell Lung cancer and (2) had completed or were still receiving treatment and 16 partners | To examine whether Mindfulness-Based Stress Reduction might be a feasible and effective intervention for patients with lung cancer and partners | Mindfulness-Based Stress Reduction | The European Organization for Research and Treatment of Cancer (EORTC) Core Quality of Life Questionnaire for Lung cancer (QLQ-LUNG CANCER 13) | No significant differences were found in Pain among the groups |
| Peddle et al, 2011, USA Exercise training (e.g., resistance training) | 17 post-treatment survivors (Mean age 66.7 yrs, 7 males, 10 females) stage I-IIIB non-small cell lung cancer (NSCLC) and limited stage small-cell lung cancer | To determine if training program would be feasible and result in improvements in objective health-related fitness as well as patient-reported outcomes | Progressive resistance exercise training | Quality of Life (QoL, SF-36) | No significant changes in patient-reported outcomes Mean change=2.9 [−0.1 to 6.4]; (p=.101) |
| Kroenke et al, 2010, USA Telecare management & symptom monitoring | 405 participants from Community Cancer Care who provide satellite oncology Breast; lung; GI; lymphoma and hematological; genitourinary& others | To determine whether centralized telephone-based care management coupled with automated symptom monitoring can improve depression and pain in patients with cancer | Tele care management (Telephonic care) Management was delivered by a nurse care manager trained in assessing symptom response and medication adherence; web or telephone based interviews were conducted to assess symptoms and in providing pain and depression specific education) | Brief Pain Inventory (BPI) | Patients in the intervention group had significantly lower pain (P_.001) and depression (P_.001) severity scores over the 12 months |
| Jane et al, 2011, Taiwan, Massage | 24 Lung cancer patients | To compare the efficacy of Massage Therapy (MT) to a social attention control condition on pain intensity, mood status, muscle relaxation, and sleep quality in a sample (n=72) of Taiwanese cancer patients with bone metastases | Standardized massage protocol for 45-minutes and direct hands-on and skin-to-skin manipulation of the soft tissue that included gentle effleurage (rhythmic, gliding strokes confirming to the contours of the body), light petrissage (lifting, rolling, kneading stroke done slowly) and compression (light compression of selected areas of tension using mild to moderate pressure), and nerve stroke (very light rushing of the skin) to target head, neck, back, and gluteus muscle, and the 4 extremities | Visual analogue scale (VAS) | Statistically significant improvement in PPI-VAS; F (1, 68)=61.17, P < 0.000, with the MT having a greater mean change difference (d=2.2, d=1.6, d=1.6) relative to the SA group (d=0.9, d=0.5, d=0.9). |
| Yeh et al, 2015, China Acupuncture (auricular point acupuncture) | 10 lung cancer patients with mean age 65 years | To examine the feasibility of an auricular point acupressure (APA) for management of pain and (2) to examine the potential APA analgesic effects for cancer patients | The auricular points selected for pain treatment included two acupoints (sympathetic and nervous subcortex) and the corresponding acupoints where patients had pain | Brief Pain Inventory (BPI) | The ‘‘average pain’’ score decreased after APA was administered and quickly reached the lowest score at day 3 (6.47 to 2.01), leading the greatest significant declination of ‘‘average pain’’ at a reduction of 69.02%. The ‘‘average pain’’ score and ‘‘pain severity’’ score significantly decreased to the lowest score at day 3, showing the greatest reduction (66.20%) after APA was used |
| Cleeland et al, 2011, USA | 79 patients, Mean age 60 years (37 males, 42 females) lung cancer or lung metastasis | To examine whether at-home symptom monitoring plus feedback to clinicians about severe symptoms contributes to more effective postoperative symptom control | Patients received automated symptom monitoring via IVR coupled with e-mail feedback to clinicians about symptoms | Symptoms were assessed using the M. D. Anderson Symptom Inventory (MDASI) | The difference in change scores between the intervention and control groups was not significant. |
| Borneman et al, 2011, USA | 72 patients, Mean age 60 years breast, lung, colon, or prostate cancers, stage III and IV disease | To test the effects of a clinical educational intervention on reducing barriers to pain and fatigue management in oncology | Trained advanced practice nurses (APN) delivered education through brochures | Karnofsky Performance Scale (KPS), Pain and Fatigue scores from Single Item Scales | Decreased pain scores for patients with pain in intervention group (Immediate effect p <0.001 , Sustained effect p 0.001) |
| Kravitz et al, 2011, USA | 201 patients, Mean age 59 years, (Males 57, Females 201) lung, breast, prostate, head and neck, esophageal, colorectal, bladder, gynecologic | to determine the effectiveness of a lay-administered tailored education and coaching (TEC) intervention | Tailored education and coaching (TEC) by health educators | Pain severity was assessed as the mean of average and worst pain, with ‘0’ on each of the two component scales representing no pain over the past 2 weeks and 10 representing the worst pain imaginable Medical Outcomes Study (MOS) Pain Impairment Scale (PIS) | No significant interaction between baseline pain severity and effect of the intervention, The effect on pain-related impairment noted at 2 weeks was not sustained at 6 and 12 weeks (P > .20,) |
RESULTS
Study selection
The initial search yielded 2288 articles. A total of 1636 references were identified for review after removal of 652 duplicates. On closer inspection, 1619 citations were excluded as they did not meet the full inclusion criteria. Twenty-three studies were selected after data extraction, including six articles obtained through cross referencing. Figure 1 illustrates the flowchart of literature search process. To be eligible for inclusion, a study must apply at least one pain measurement before and following the intervention or should have measured pain after the intervention, which was our only outcome we considered.
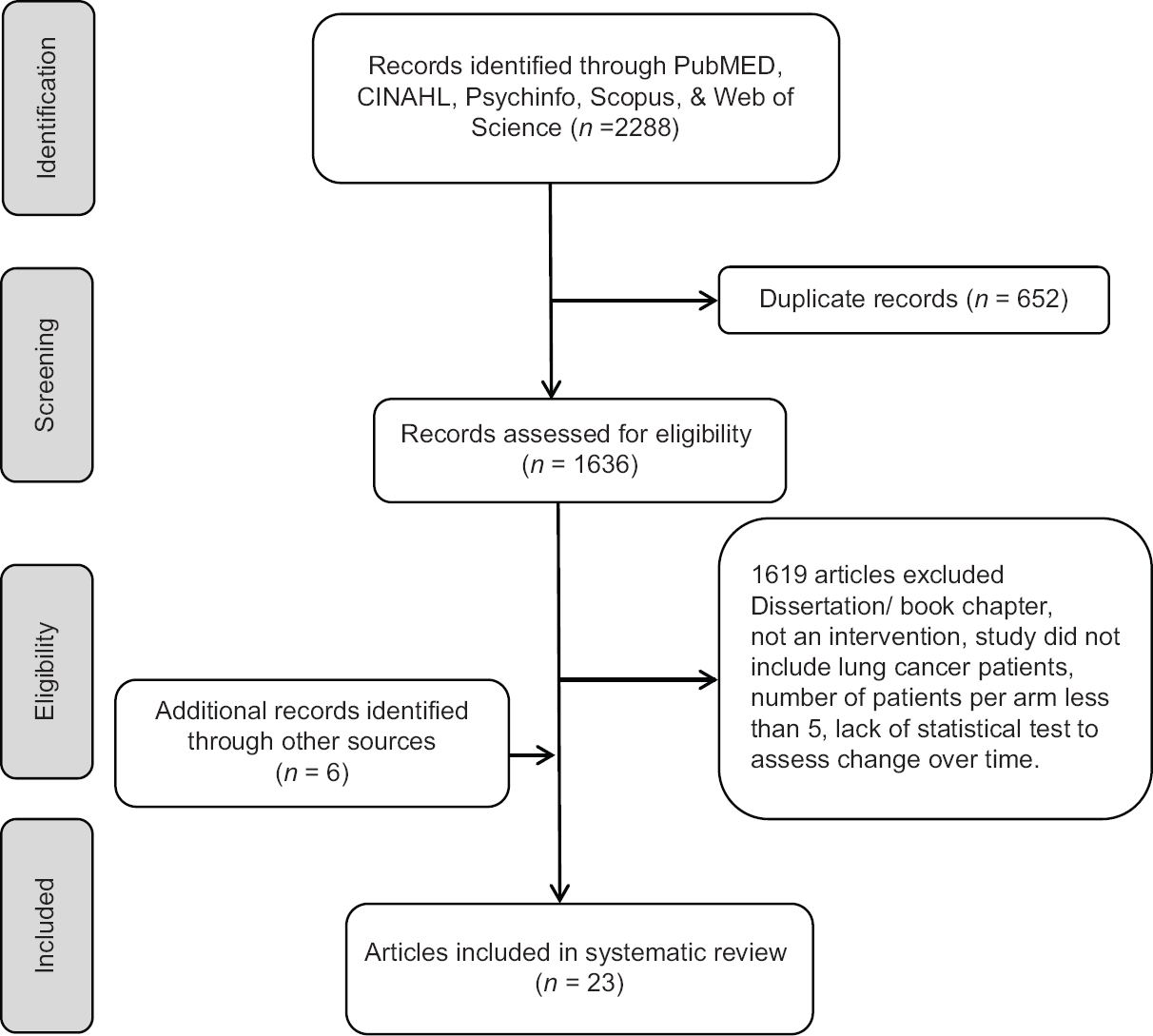
- Flowchart of literature search for non-pharmacological interventions for pain management in lung cancer
Characteristics of nonpharmacological interventions
Participants
The main characteristics of the reviewed studies are summarized in Table 1. The majority of studies were conducted in the US (n = 14), however, other locations included Canada (n = 2), Denmark (n = 1), Germany (n = 3), The Netherlands (n = 1), Spain (n = 1), Taiwan (n = 1), and the UK (n = 1). Out of the 22 studies included in this systematic review,[171819202122232425262728293031323334353637383940] ten involved only participants with lung cancer [Table 1]. In total, this review included 6315 participants, with sample size per study ranging from 17 to 3133 participants. Gender distribution was reported in all but two studies.[2324] The average male percentage cohort was 61%. All studies included adults, with age ranging from 18 to 75 years.
Classification of interventions
In this study, nonpharmacological interventions were broadly classified into five categories:
-
Physical treatment interventions
-
Self-management and coaching interventions
-
Cognitive behavioral interventions
-
Technology-based interventions
-
Coping skills interventions.
Of the six studies that emphasized physical treatment, four focused on physical exercise activity and physical therapy,[18212433] two studies focused on massage,[2532] whereas one study focused on acupressure.[40] Five studies were concerned primarily on enhancing cognitive and coping skills.[2930343537] Four studies centered on self-management and coaching.[17273941] Well-being and mindfulness interventions were the focus of three studies.[233138] Three studies centered on the utilization of technology such as telephone or Internet to enhance symptom control.[202842]
Nature of interventions
Among physical treatment interventions, exercise treatments were the most examined.[18212433] Exercise interventions were delivered in either a group format[18] or individual sessions.[212433] The comparison groups received individualized sessions of home exercise instructions and postsurgery counseling[18] and conventional physiotherapy including breathing techniques, massage, muscle stretching, and distraction.[24] There were no control groups in two studies.[2133] One intervention considered massage therapy[25] consisting of standardized massage and manipulation of soft tissue, whereas one intervention combined massage with exercise.[32] The control group received either social attention[25] or simple hand touch.[32] A second intervention without a control group involved an acupressure intervention which was delivered by Yeh et al.[40] This modality involved sessions where participants received 7 days of brief acupressure treatment for their pain.
In a pretest and posttest one group design, Kwekkeboom et al. evaluated the effect of in-person delivered strategies for relaxation, imagery, and distraction exercises for pain and other symptoms.[29] No control group was used in this intervention. The same cognitive-behavioral intervention was used in a RCT[30] where the control group received usual care. Two interventions evaluated the efficacy of caregiver-assisted coping skills training (CST) and brief pain coping skills training (PCST) interventions delivered via telephone or videoconference.[3437] One study provided participants with a combined one-on-one session of narrative therapy and anti-depressant medication,[35] whereas the usual care group received an anti-depressant medication and information about medication.
Four studies involved self-management and coaching interventions.[17273941] In one study, participants received four educational sessions (“Passport to Comfort”) on minimizing barriers to pain and fatigue, whereas the control received standard care.[17] In another study, a combination of education and coaching sessions aimed to reduce misconceptions about pain and improving self-efficacy in communicating pain to physicians by patients receiving the intervention, whereas those in the control group received enhanced care.[39] The feasibility of Pro-SELF Plus Pain Control Program was evaluated when delivered on a one-on-one basis over 6 1-h sessions.[27] The control group received standard education and care. In the remaining study, Wilkie et al. (2010) evaluated the effects of sensory self-monitoring and reporting coaching of pain in the intervention group, whereas the control group discussed cancer experiences.[39]
Among the technology-based interventions,[202842] the first one utilized a telephone-based management care coupled with an automated monitoring of symptoms. The second administered a web-based Internet platform intervention.[28] The remaining two interventions assessed the efficacy of routine screening for distress program to assist patients on physical and psychosocial symptoms including pain, fatigue, anxiety, and depression.[2042] Three variants of a routine screening for distress[20] included the minimal screening (usual care and distress level screening), full screening (minimal screening, screening for distress symptoms, and tailored report of patient's concerns), and triage screening (full screening and referral to patient's medical choice as founded appropriate by a member of psychosocial team). Similar to the previous intervention, Carlson et al. compared the impact of a computerized triage intervention that provides participants with a tailored printout summarizing participant's concerns and access instructions to appropriate services to a personalized triage that provides participants with the same printout summary, but participants are contacted to discuss referral options.[42]
Delivery of interventions
A face-to-face approach was the main interventional element of 17 studies.[1721232425262729303132333536384043] Three interventions were delivered to participants on the computer.[203742] A telephone-based intervention was used in three studies.[222834] One study used a combination of video, written materials, and in-person, mail or phone delivery intervention elements.[39]
Outcomes
All 23 studies included in this systematic review assessed pain intensity or pain severity. The brief pain inventory (BPI) which assessed pain severity was used in seven studies.[28293032343740] A single- or two-item Numeric Rating Scale were used in six interventions.[172021262742] Two studies measured Present Pain Intensity with a Visual Analogy Scale.[2539] While Rodríguez et al. used the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ C-30)[35] and van den Hurk et al. used The EORTC QLQ Lung Cancer,[38] Henke et al. used both questionnaires.[24] Other instruments used were Medical Outcomes Studies Short-Form General Health Survey-36;[31] and 36-Item Short Form Health Survey (RAND SF-36);[2333] McGill-Pain Questionnaire;[39] and MD Anderson Symptom Inventory.[22] Other outcomes included pain frequency, pain interferences, bodily pain, and pain location [Table 1].
RESULTS OF THE INTERVENTIONS
Exercise interventions yielded mixed results.[18212433] Brocki et al. (2014) evaluated the effects of a group supervised intervention and reported a moderate, but significant decrease in bodily pain that was short-term (4-month follow-up; mean difference 15.3, 95% confidence interval [CI]: 4–26.6, P = 0.01), but the effect was not sustained long-term (12-month follow-up; P = 0.49).[18] Another program that focused on strength training developed and evaluated a rapid, easy, and strength training exercise program as part of a multidisciplinary intervention.[21] The program did not improve participants' pain scores overtime compared to those in the control group (P = 0.87). Similarly, the supervised resistance exercise training conducted by Peddle-McIntyre et al. found that participants did not decrease their bodily pain levels over 12 weeks (mean difference: 2.9, 95% CI: −0.1–6.4, P = 0.101).[33] Similarly, participants receiving a 7-day strength and endurance training program[24] did not diminish pain levels compared to those in the control group (P > 0.05). However, a differential effect was observed in terms of reported pain location, where participants' pain in their arms or shoulder (P = 0.048) improved significantly, but not for chest and other body parts.[24]
Both interventions that considered massage therapy as an intervention whether entirely or combined with physical exercise yielded significant improvement in the pain level among participants. In one study that evaluated three consecutive massages,[25] participants reported an immediate beneficial effect after each session compared to the control group at each time point (all P < 0.001) and it reached clinical significance over time (F 1 68) =61.17, P < 0.001). However, mean pain scores between the two groups converged overtime (P = 0.41).[25] In the other study, combined massage therapy with exercise[32] improved participants' pain scores compared to controls for BPI worst pain (mean difference: −1.5, 95% CI: −3.08, −0.008), BPI current pain (mean difference: −2.0, 95% CI: −3.9, −0.1), and total BPI index (mean difference: −2.68, 95% CI: −4.17, −1.18), but not for BPI least pain and BPI pain on average (all P > 0.127). The analgesic effect of acupressure on cancer pain management was shown to yield a short-term reduction in pain intensity, pain average, pain severity, and pain interference of >60% and 50% after the first session (i.e., 3 days from baseline) and at the end of 7 days, respectively (all P < 0.001).[40]
A patient-controlled cognitive behavioral (PC-CB) intervention including strategies for relaxation and imagery exercises[29] yielded significant immediate changes (1-week) in participants' mean pain severity scores (pretest: 4.54 ± 2.27 vs. post-test: 2.77 ± 2.06, P < 0.01), but pain ratings made before and after the 2-week intervention did not differ from each other. One RCT that delivered the same PC-CB intervention but to a larger sample of cancer patients,[30] showed immediate pre- to posttreatment (1 week) changes in pain severity scores (P < 0.001). Moreover, at the 2-week follow-up, pain severity scores in the PC-CB group improved significantly compared to those in the control group (P < 0.006).[30]
The two coping skills interventions had similar results. Porter et al. (2011) assessed the efficacy of a cognitive behavioral intervention in lung cancer patients by comparing a caregiver-assisted CST protocol to an education/support intervention.[34] The results indicated that the participants in both groups improved their worst pain scores over 6 months (P < 0.002).[34] Similarly, a brief PCST intervention[37] (Sommers et al., 2015) was shown to reduce pain after a 1-week intervention (pretreatment: 4.75 ± 1.97; posttreatment: 3.37 ± 1.63; t = 2.92, P = 0.009).
A RCT assessed the combined effect of a psychotherapeutic intervention such as narrative therapy with pharmaceutical treatment (e.g., escitalopram) by comparing it to usual care and escitalopram treatment.[35] A significant pain reduction in the combined therapy group (mean difference: 17.86, 95% CI: 17.86–37.69) compared to the usual care (16.16, 95% CI: 5.35–26.94) was detected at 12 months and 24 months, respectively (combined therapy: 24.24, 95% CI: 13.5–35; usual care: 44.87, 95% CI: 34.9–54.8). Overall, the combined intervention was beneficial in reducing pain overtime compared to the usual care and escitalopram treatment (P = 0.002).
The self-management and coaching interventions saw mixed results. Borneman et al. (2015) evaluated the effectiveness of “Passport to Comfort,” an educational intervention to improve pain and fatigue management in cancer patients when compared to the control group (i.e., usual care).[17] While an immediate effect in pain change at 1-month follow-up (all P < 0.007) was detected in both groups (intervention and control groups), a sustained effect at 3-month follow-up was detected only in the intervention group (P = 0.001). A tailored education and coaching intervention to minimize misconceptions related to pain and improving self-efficacy of communicating pain to physicians,[27] briefly improved pain-related functional impairment at 2 weeks (P = 0.01), but this effect was not sustained overtime at 6 and 12 weeks (when compared to the control group). In addition, there were no statistically significant changes in pain severity between patients who received the intervention and those in the control group at any time points (all P > 0.27). A pain self-management intervention of skills building, information provision and coaching[26] did not improve the average and worst pain scores of participants at 10 and 22 weeks (all P > 0.48). Similarly, coaching patients to communicate pain to their providers did not improve participants' pain intensity and pain relief scores at 4-week follow-up (all P > 0.37).
Among the mindfulness and well-being interventions, 3 months of choral singing was reported to improve bodily pain of cancer survivors, (pretest: 62.1 ± 28.8; posttest: 72.9 ± 28.2, P = 0.01) where higher scores indicate lesser pain.[23] Similarly, a mindfulness-based stress reduction program that included meditation and yoga sessions,[31] and an intervention that encouraged meditation and a silent day improved patients' pain scores directly after and 3 months after the Mindfulness-Based Stress Reduction training.[38]
Of the three technology-based interventions, telecare management coupled with an automated symptom monitoring system was found to be efficacious in reducing pain.[28] Pain severity decreased significantly in participants receiving the intervention compared to controls at each time point (e.g., 3, 6, and 12 months; all P < 0.01). The largest moderate effect size for between-groups difference was detected immediately after the intervention; however, the effect size remained moderate although slightly attenuated but statistically significant at 6 and 12 months. Other pain-specific outcomes, including pain interference and bodily pain scores improved significantly over 12 months in the intervention group compared to the control group.[28] The remaining two interventions assessed the efficacy of routine screening for distress program to assist patients on physical and psychosocial symptoms including pain, fatigue, anxiety, and depression.[2042] Among the three variants of a routine screening distress program [Table 1], patients in the triage group benefited the most by reporting the presence of pain and of clinically elevated pain level (≥4) less frequently (32%) at 3 months compared to those in the minimal screening group (all P < 0.04), but not when compared to full screening group. However, all three groups exhibited similar mean Pain Thermometer levels (P = 0.142). In addition, participants from the triage group were more frequently referred to psychosocial resources than the full screening and minimal screening groups (P = 0.001) and when compared to those nonreferred, they did not improve pain overtime (P = 0.26). Overall, the triage screening and full screening equally decrease the level of pain of participants overtime (P = 0.42). Carlson et al. further explored the efficacy of the triage screening for distress by comparing personalized versus a computerized triage version.[42] While both interventions decreased participants' pain levels over time, there was a significant decline in the rate of change over time for pain along with other clinical symptoms (P < 0.0001). In addition, a moderate change in pain was also observed among patients in the personalized group (0.52 standard deviation [s.d.]) compared to a smaller reduction in pain for the computerized group (0.33 s.d.).
DISCUSSION
This systematic review was done to compare the efficacy of nonpharmacological interventions in reducing pain in lung cancer patients. Pain is a multifaceted phenomenon and is a result of interactions between biological, affective, cognitive, behavioral, and sociocultural.[44] A pharmacological approach for pain management is considered the standard in clinical settings. Yet, it does not deliver reliable pain control in cancer patients.[1345] This is a significant problem as the prevalence of pain in lung cancer patients is estimated to be >45%.[7] Thus, aside from interventions that address the biological aspect of pain, nonpharmacological interventions have been recommended by agencies such as the World Health Organization as adjuvants for pain management.[46]
A systematic review of the effects of such interventions was conducted between 2010 and 2013 in patients exhibiting various types of cancer[13] and the findings indicated the effectiveness of the interventions was rather limited with only a short-term effect. We expanded on this knowledge and examined the effects of nonpharmacological interventions for pain management targeting lung cancer patients. To our knowledge, such a systematic review has not been carried out previously in this oncologic population.
The present systematic review included 23 interventions classified into several categories including physical treatment, technology-based, cognitive behavioral training, coaching, and well-being. While heterogeneity in results was detected among each category of interventions, the majority of them had some short-term pain-relieving effect. There was some evidence of short-term benefit for the relief of cancer pain with almost all interventions, viz a viz., physical exercise activity and physical therapy, massage, cognitive and coping skills, self-management and coaching. Well-being and mindfulness intervention and the utilization of technology to enhance pain control are still in infancy. Thus, due to the heterogeneous nature of the samples and lack of sufficient power and a paucity of rigorous trials, no interventions can be recommended currently.
Exercise interventions were one of the most frequently cited in this systematic review [Table 1], yet they yielded mixed results. In this review, the two interventions that were effective, pain subsided after a short-term exercise regimen,[2443] whereas the other two studies did not report any significant effects.[2133] This finding is similar to the mixed results that were reported in a systematic review conducted in breast cancer patients to assess the efficacy of exercise in alleviating pain.[47]
Therapeutic massage as a cancer pain intervention appears to be safe and effective and the use of massage in cancer care centers and hospitals is on the rise.[48] This finding is similar to the conclusions of some of the previous studies for other areas of cancer.[4950] It is believed that the actual benefits of massage therapy are a combination of many factors such as the communication between the masseuse and the individual, the massage therapists' “personal touch,” and the patients' attitude about the therapy and the particular technique of massage.[51] Our review also identified the benefit of physical therapy. This intervention can be an effective augment to regular analgesic medication.[52] Literature related to beneficial effects of massage therapy are scanty. The postulated mechanism of the therapy is to relax the muscles and nerves which help to reduce pain associated with contractions or spasms. Massage therapy also are known to benefit neural tissues by reducing compression of the nerves. One study showed that incorporating the massage therapy in regular care of patients with acute conditions helps the patient positively to cope with the physical and mental trauma.[25]
Patient empowerment has been associated with controlling life by adopting the concepts of self-efficacy participating actively and increasing one's own abilities to face challenges.[53] Many models have been tested to enable and empower the individual patients and caregivers in a custom-made way that is preferred by themselves.[54] On the contrary, one study showed that patient empowerment led to an improved quality of care regarding postoperative pain but did not shorten the postoperative pain in old patients who had undergone surgery for cancer.[36] Unfortunately, there is still confusion regarding the operationalization of patient empowerment and issues related to the validity and reliability measures.
Among all cited interventions, there is evidence that cognitive behavioral and coping interventions alleviate pain. The cognitive behavioral approach is useful for modifying the coping skills in varied groups. Another brief review compared patient psycho-education, supportive psychotherapy, and cognitive-behavioral interventions among cancer patients and concluded that a combination of traditional health services and psychosocial support are classic examples of care which is comprehensive and integrated.[55] This conclusion has to be still verified in lung cancer patients exclusively. Similarly, in one of the included studies, the effect detected predominantly was immediate, but it was sustained.[35] Coping strategies for pain due to cancer are still not widely accepted and used due to the lack of sufficient empirical evidence.[56] Nonetheless, coping strategies may be a significant method of alleviating pain among cancer patients and survivors.
Mindfulness-based interventions can be considered as an effective way for functional improvements among cancer survivors.[57] Our review also noted the significant improvements in pain perception by the patients. One meta-analysis concluded that Mindfulness based stress reduction might not only help in reducing pain but also in improving the psychosocial aspects by allowing them to adjust to their status.[58]
Acupressure has also been used with some degree of success. In our review we identified a study which used acupressure therapy for 7 days.[40] Most of the time, this therapy is actually used to prevent nausea and cough caused due to the side effects of other medication for cancer treatment.
Technology-based interventions utilized either the web Internet interface or telephonic reminders. In our review, we found that telecare management was very efficient.[28] New strategies are being developed to use mobile-based interventions in these patients. This will potentially help health-care professionals and providers to maintain and manage the patients remotely.[59]
The above nonpharmacological interventions potentially offer a ray of hope to cancer patients suffering from pain. Providing better access, awareness, and coordinating with different stake holders in health care can be a very effective measure in improving patient experience. Future studies should strive to conduct more stringent RCTs to establish the potential use of these interventions in various settings and ultimately provide timely and appropriate relief to lung cancer patients.
Several limitations should be noted, however. First, the sample size of most of the studies was small and heterogeneous leading to underpowered effect size among the interventions. Fourteen studies had small sample sizes (n = 17–86), and only 8 studies had >200 participants (n = 201–3133). Second, the length of interventions varied from short periods of time (3 days to 2 weeks) to a longer periods of time (e.g., 1–4 months). Only few studies had subsequent follow-ups.[2728323538414243] Third, some studies lacked a control group which maximizes the threat for potentially confounding variables, thus reducing a study's internal validity.[1723293133373840] Fourth, a variety of outcome measures were used in these interventions (e.g., pain interference, pain severity, pain frequency, and pain location) thus, making it difficult to compare results between studies and to assess clinical significance of findings even when statistical significance was achieved. Finally, participants varied in their cancer stage and level of pain reported at the entrance in the study which adds to the layer of difficulty of comparing and contrasting results between studies.
CONCLUSIONS
The findings from this systematic review suggest that nonpharmacological interventions may have beneficial effects in alleviating pain in lung cancer patients. However, more research is warranted to explore the long-term effect of such interventions on pain management in this oncologic population. One recommendation involves the use of control groups and larger sample sizes to adequately control for potential confounders of pain which will allow a more robust analyses of the effect of nonpharmacological interventions on pain. Most interventions that exhibited pain alleviating benefits were short-term; however, whether these interventions have sustained benefits could be assessed by extending the follow-up periods.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Symptom prevalence, intensity, and distress in patients with inoperable lung cancer in relation to time of death. J Clin Oncol. 2007;25:5381-9.
- [Google Scholar]
- Symptom prevalence, distress, and change over time in adults receiving treatment for lung cancer. Psychooncology. 2003;12:694-708.
- [Google Scholar]
- Prevalence and management of pain in Italian patients with advanced non-small-cell lung cancer. Br J Cancer. 2004;90:2288-96.
- [Google Scholar]
- Symptom burden and quality of life in advanced non-small cell lung cancer patients in France and Germany. Lung Cancer. 2013;81:288-93.
- [Google Scholar]
- Pain, fatigue, disturbed sleep and distress comprised a symptom cluster that related to quality of life and functional status of lung cancer surgery patients. J Clin Nurs. 2013;22:1281-90.
- [Google Scholar]
- Pain experienced by lung cancer patients: A review of prevalence, causes and pathophysiology. Lung Cancer. 2004;43:247-57.
- [Google Scholar]
- Clinical management of pain in advanced lung cancer. Clin Med Insights Oncol. 2012;6:331-46.
- [Google Scholar]
- Management of cancer pain: ESMO Clinical Practice Guidelines. Ann Oncol. 2012;23(Suppl 7):vii139-54.
- [Google Scholar]
- A review of potential adverse effects of longterm opioid therapy: A practitioner's guide.PRIM care companion. CNS Disord. 2012;14:1-14.
- [Google Scholar]
- Nonpharmacological therapies in pain management. In: Gabor BR, Carl EN, eds. Pain Management-Current Issues and Opinions. Rijeka, Croatia: InTech; 2012. p. :485-502.
- [Google Scholar]
- A systematic review: Non-pharmacological interventions in treating pain in patients with advanced cancer. J Adv Nurs. 2014;70:1954-69.
- [Google Scholar]
- Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1.
- [Google Scholar]
- AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
- [Google Scholar]
- The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377-84.
- [Google Scholar]
- Support for patients and family caregivers in lung cancer: Educational components of an interdisciplinary palliative care intervention. J Hosp Palliat Nurs. 2015;17:309-18.
- [Google Scholar]
- Improvements in physical performance and health-related quality of life one year after radical operation for lung cancer. Cancer Treat Commun. 2015;4:65-74.
- [Google Scholar]
- Screening for distress, the sixth vital sign, in lung cancer patients: Effects on pain, fatigue, and common problems–secondary outcomes of a randomized controlled trial. Psychooncology. 2013;22:1880-8.
- [Google Scholar]
- Online screening for distress, the 6th vital sign, in newly diagnosed oncology outpatients: Randomised controlled trial of computerised vs personalised triage. Br J Cancer. 2012;107:617-25.
- [Google Scholar]
- A home-based exercise program to improve function, fatigue, and sleep quality in patients with Stage IV lung and colorectal cancer: A randomized controlled trial. J Pain Symptom Manage. 2013;45:811-21.
- [Google Scholar]
- Automated symptom alerts reduce postoperative symptom severity after cancer surgery: A randomized controlled clinical trial. J Clin Oncol. 2011;29:994-1000.
- [Google Scholar]
- A pilot investigation of quality of life and lung function following choral singing in cancer survivors and their carers. Ecancermedicalscience. 2012;6:261.
- [Google Scholar]
- Strength and endurance training in the treatment of lung cancer patients in stages IIIA/IIIB/IV. Support Care Cancer. 2014;22:95-101.
- [Google Scholar]
- Effects of massage on pain, mood status, relaxation, and sleep in Taiwanese patients with metastatic bone pain: A randomized clinical trial. Pain. 2011;152:2432-42.
- [Google Scholar]
- Results of a randomized controlled pilot study of a self-management intervention for cancer pain. Eur J Oncol Nurs. 2013;17:284-91.
- [Google Scholar]
- Cancer Health Empowerment for Living without Pain (Ca-HELP): Effects of a tailored education and coaching intervention on pain and impairment. Pain. 2011;152:1572-82.
- [Google Scholar]
- The association of depression and pain with health-related quality of life, disability, and health care use in cancer patients. J Pain Symptom Manage. 2010;40:327-41.
- [Google Scholar]
- Feasibility of a patient-controlled cognitive-behavioral intervention for pain, fatigue, and sleep disturbance in cancer. Oncol Nurs Forum. 2010;37:E151-9.
- [Google Scholar]
- Pilot randomized controlled trial of a patient-controlled cognitive-behavioral intervention for the pain, fatigue, and sleep disturbance symptom cluster in cancer. J Pain Symptom Manage. 2012;44:810-22.
- [Google Scholar]
- Mindfulness based stress reduction in post-treatment breast cancer patients: An examination of symptoms and symptom clusters. J Behav Med. 2012;35:86-94.
- [Google Scholar]
- Effects of physical therapy on pain and mood in patients with terminal cancer: A pilot randomized clinical trial. J Altern Complement Med. 2012;18:480-6.
- [Google Scholar]
- Feasibility and preliminary efficacy of progressive resistance exercise training in lung cancer survivors. Lung Cancer. 2012;75:126-32.
- [Google Scholar]
- Caregiver-assisted coping skills training for lung cancer: Results of a randomized clinical trial. J Pain Symptom Manage. 2011;41:1-3.
- [Google Scholar]
- Combined therapy versus usual care for the treatment of depression in oncologic patients: A randomized controlled trial. Psychooncology. 2011;20:943-52.
- [Google Scholar]
- Patient empowerment improved perioperative quality of care in cancer patients aged ≥65 years – A randomized controlled trial. PLoS One. 2015;10:E0137824.
- [Google Scholar]
- A pilot study of a mobile health pain coping skills training protocol for patients with persistent cancer pain. J Pain Symptom Manage. 2015;50:553-8.
- [Google Scholar]
- Mindfulness-Based Stress Reduction for lung cancer patients and their partners: Results of a mixed methods pilot study. Palliat Med. 2015;29:652-60.
- [Google Scholar]
- Effects of coaching patients with lung cancer to report cancer pain. West J Nurs Res. 2010;32:23-46.
- [Google Scholar]
- Auricular point acupressure as an adjunct analgesic treatment for cancer patients: A feasibility study. Pain Manag Nurs. 2015;16:285-93.
- [Google Scholar]
- A systematic evaluation of content, structure, and efficacy of interventions to improve patients' self-management of cancer pain. J Pain Symptom Manage. 2012;44:264-84.
- [Google Scholar]
- Screening for distress and unmet needs in patients with cancer: Review and recommendations. J Clin Oncol. 2012;30:1160-77.
- [Google Scholar]
- Short and long-term effects of supervised versus unsupervised exercise training on health-related quality of life and functional outcomes following lung cancer surgery – A randomized controlled trial. Lung Cancer. 2014;83:102-8.
- [Google Scholar]
- The role of psychological interventions in the management of patients with chronic pain. Psychol Res Behav Manag. 2011;4:41-9.
- [Google Scholar]
- Non-pharmacological cancer pain interventions in populations with social disparities: A systematic review and meta-analysis. Support Care Cancer. 2016;24:985-1000.
- [Google Scholar]
- Individual patient treatment use of unapproved drugs: A new option for the seriously ill. J Pain Palliat Care Pharmacother. 2010;24:19-22.
- [Google Scholar]
- The efficacy of exercise therapy in reducing shoulder pain related to breast cancer: A systematic review. Physiother Can. 2013;65:321-30.
- [Google Scholar]
- Massage therapy as a supportive care intervention for children with cancer. Oncol Nurs Forum. 2008;35:431-42.
- [Google Scholar]
- Foot and hand massage as an intervention for postoperative pain. Pain Manag Nurs. 2004;5:59-65.
- [Google Scholar]
- Massage therapy for cancer patients: A reciprocal relationship between body and mind. Curr Oncol. 2007;14:45-56.
- [Google Scholar]
- Cancer Pain: A critical review of mechanism-based classification and physical therapy management in palliative care. Indian J Palliat Care. 2011;17:116-26.
- [Google Scholar]
- Patient empowerment in cancer pain management: An integrative literature review. Psychooncology. 2014;23:1203-11.
- [Google Scholar]
- Self-management: Enabling and empowering patients living with cancer as a chronic illness. CA Cancer J Clin. 2011;61:50-62.
- [Google Scholar]
- Nonpharmacological interventions with chronic cancer pain in adults. Cancer Control. 2000;7:157-64.
- [Google Scholar]
- Integrating mindfulness in supportive cancer care: A cohort study on a mindfulness-based day care clinic for cancer survivors. Support Care Cancer. 2015;23:2945-55.
- [Google Scholar]
- Mindfulness-based stress reduction and cancer: A meta-analysis. Psycho-oncology. 2009;18:571-9.
- [Google Scholar]
- Feasibility of a mobile and web-based intervention to support self-management in outpatients with cancer pain. Eur J Oncol Nurs. 2016;23:97-105.
- [Google Scholar]




