
Translate this page into:
Supportive and Palliative Care Needs of the Older Adults with Stroke and Neurological Diseases: An Estimation using data from Longitudinal Ageing Study in India
*Corresponding author: Benson Thomas M, School of Public Health, SRM Medical College Hospital and Research Centre, Chennai, Tamil Nadu, India. bensontm@srmist.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Immanuel T, Salins N, Sundararaj J, Gursahani R, Thomas MB. Supportive and Palliative Care Needs of the Older Adults with Stroke and Neurological Diseases: An Estimation using Data from Longitudinal Ageing Study in India. Indian J Palliat Care. 2024;30:322-9. doi: 10.25259/IJPC_20_2024
Abstract
Objectives:
The prevalence and burden of neurological diseases are high among the older age group. Stroke and other neurological diseases significantly impair functional capacity and lead to poor quality of life. This study aims to provide a national-level estimate for palliative and supportive care needs among older Indian adults with stroke and other neurological diseases.
Materials and Methods:
The Longitudinal Ageing Study in India (LASI), a national-level survey of older adults, was used as a representative sample to estimate palliative and supportive care needs. The supportive and palliative care indicator tool income setting (SPICT-LIS) was used to identify palliative care needs in older adults with stroke and other neurological diseases. A total of 31,902 older adults aged 60 years and above were identified from the LASI data, and among them, 1458 older adults with stroke and other neurological diseases were selected for the analysis. The SPICT-LIS indicators were compared with the selected LASI data. Both univariate analysis and multivariate logistic regression were performed to determine the association between supportive and palliative care needs and background characteristics of older adults.
Results:
The analysis showed that 63.6% of older adults with stroke and other neurological diseases in India have supportive and palliative care needs. In regression analysis, the burden of supportive and palliative care needs was observed to be high among older adults who were in the underweight, overweight/obese category, who experienced ill-treatment, and who had diabetes and hypertension. In contrast, the burden of supportive and palliative care needs was observed to be low among older adults with stroke and neurological diseases who belonged to richer and richest economic quintiles, those receiving at least one social support scheme, those engaged in social activity and those performing physical activity.
Conclusion:
The palliative care needs among the older adult population with stroke and other neurological diseases in India are high. The findings of this study underscore the importance of screening for supportive and palliative care needs among patients with stroke and other neurological diseases to identify these unmet needs. The workforce trained in the provision of generalist and specialist palliative care will be required to meet this need, and the population of older adults is estimated to double in the next three decades.
Keywords
Stroke
Neurological diseases
Supportive and palliative care
Supportive and palliative care indicator tool income setting
Older adults

INTRODUCTION
The increasing share of the older population necessitates the need for proactive supportive and palliative care.[1] According to the World Health Organization (WHO), one in six people will be more than 60 years old globally by 2030, and by 2050, the population above 60 years of age is estimated to increase to 2.1 billion from 1 billion in 2020.[2] Meanwhile, among those aged 80 years and above, the population size is expected to triple by 2050 from what it was in 2020.[3] The ageing process of older adults results in increased susceptibility to deteriorating physical and mental health, non-communicable and degenerating diseases, falls and injuries leading to disabilities, dependencies and deaths.[4-6] The Lancet Commission reports that, globally, serious health-related suffering (SHS) for older adults who are more than 70 years of age will increase rapidly to up to 183% by 2060 from its estimates of the year 2016.[7] The report also states that the burden of SHS will rise even more rapidly among older adults in low-income countries.[7] The WHO estimates that 58 million people, including 25.7 million in the last year of their lives, will require palliative care every year.[8] However, only 14% of them are receiving palliative care.[8]
India is not exempt from this growth in ageing population and high supportive and palliative care needs.[9,10] According to current estimates, by 2025, India’s older population will reach 158.7 million.[11] This number will more than double to 347 million by 2050, taking a 20% share of the Indian population, accompanied by a high rise in the burden of chronic illnesses, disability and dependence in the country.[11] Consequently, there will be SHS associated with chronic diseases.[7] Palliative care is an approach that aims to reduce serious SHS.[12] However, only <2% of the Indian population has access to palliative care.[13] One of the significant challenges in access to palliative care is identifying patients with palliative care needs.[14] In India, few studies have been carried out to estimate the palliative care needs of the local population.[15-18] These estimates are based on the general population living in the micro-level localities where the older adults are not adequately represented. With the growing older population in India, there is a great need to provide palliative care estimates to develop policies and implement programs to meet their needs.
Among the different conditions that require palliative care, neurological diseases are observed to be more prevalent among the older adult age group.[19] Stroke and other neurological diseases significantly impair functional capacity and are associated with poor quality of life. However, the neuro-palliative care needs of the Indian senior population are largely unknown. This paper aims to provide a national-level estimate for palliative and supportive care needs among Indian older adults with stroke and other neurological diseases based on Longitudinal Ageing Study in India (LASI) data, a nationally representative sample survey of the Indian senior population.
MATERIALS AND METHODS
We used the supportive and palliative care indicator tool low-income setting (SPICT-LIS), a validated instrument to identify patients with palliative care needs. The Primary Palliative Care Research Group, University of Edinburgh, developed the tool in 2010. [20,21] The tool provides general indicators of poor or deteriorating health for all patients and specific indicators for eight different health conditions to identify patients with palliative care needs. In this study, we used the indicators from ‘SPICT-LIS’ to assess the palliative requirement for stroke and other neurological conditions. Subsequently, these indicators were mapped on the survey data from LASI to identify the older adults who required palliative care for stroke and other neurological diseases.
The LASI is a nationally representative survey of 73,396 older adults aged 45 and above across all states and union territories of India.[22] Although the LASI was envisioned to be a longitudinal survey to be conducted every 2 years, the first wave of the LASI survey carried out between April 2017 and December 2018 is cross-sectional in nature.[22] The survey adopted a multistage stratified area probability cluster sampling design to choose its samples. The survey used a standardised tool with quality controls to minimise non-sampling errors. The objective of the LASI was to provide comprehensive information based on demographics, economic status, chronic conditions, experience of medical symptoms, functional status, mental health (cognition and depression), health insurance status, healthcare utilisation and life expectations.[22] This study included older adults who are aged 60 years and above with stroke and other neurological diseases in the estimation process.
Figure 1 depicts the mapping of ‘SPICT-LIS’ indicators about stroke and neurological diseases with that of LASI. According to the ‘SPICT-LIS’ criteria, four indicators must be considered for the palliative requirement. The first indicator is progressive deterioration in physical and cognitive function despite available therapy that was matched in LASI data variables as the inability to perform activities of daily living such as dressing, eating, bathing and toileting due to their physical and memory problems. The second indicator of ‘SPICT-LIS’ is ‘increasing difficulty speaking and progressive swallowing difficulties’, which was mapped with the LASI variable as Having difficulty in speaking and Swallowing. Episodes of aspiration pneumonia, breathlessness or respiratory failure were the third indicator mapped with LASI data. Although shortness of breath while awake and others were available in LASI, these questions were not considered as they may not be relevant in stroke and neurological diseases. The fourth indicator of ‘SPICT-LIS’ was ongoing severe disability after stroke despite the best available rehabilitation, which correlated with persistent weakness in the arms and legs, decreased ability to move, difficulty in vision and thinking and difficulty in finding words due to stroke in LASI.
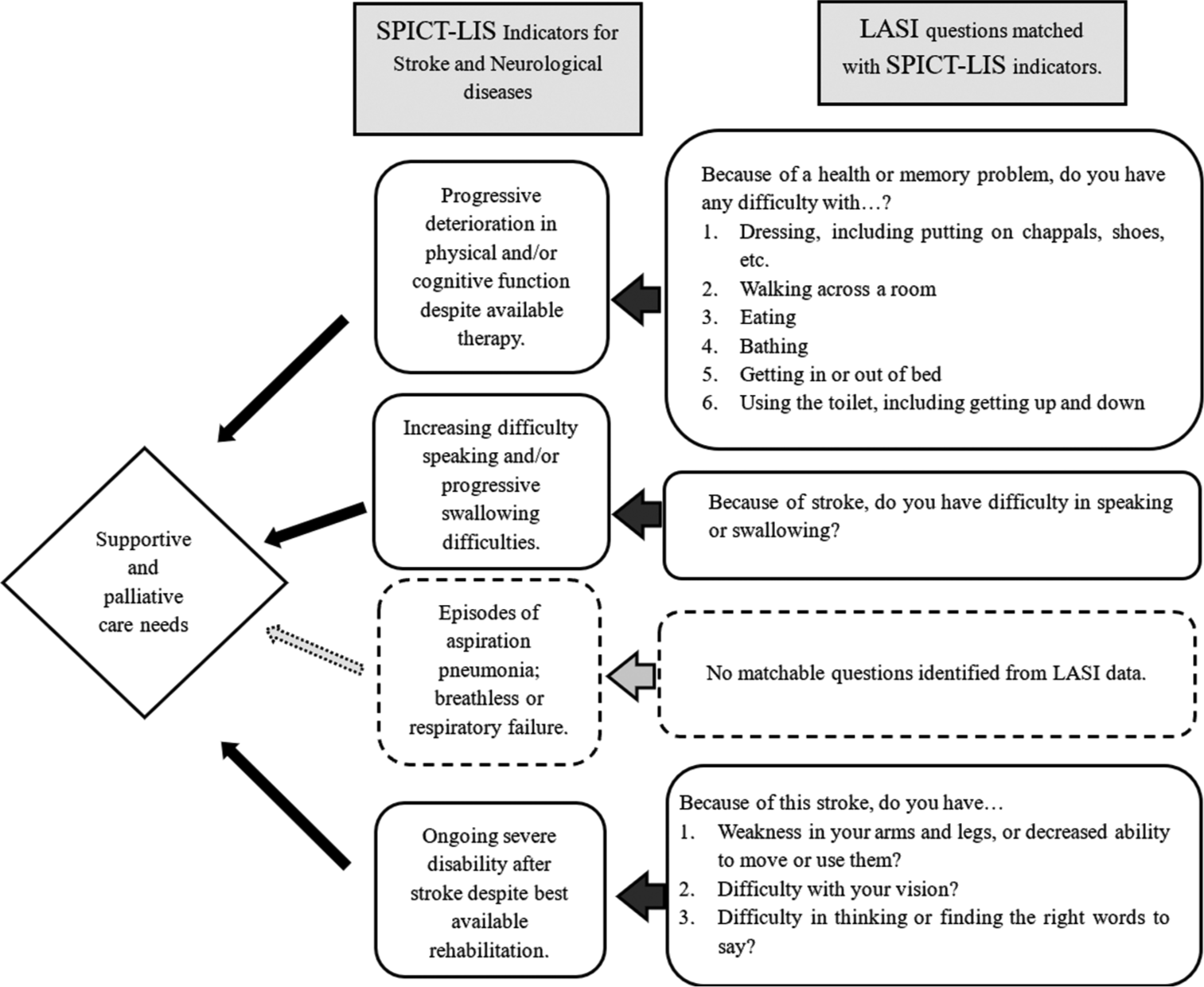
- Framework for identifying older adults with supportive and palliative care needs due to stroke and other neurological diseases using supportive and palliative care indicator tool (SPICT)-low-income settings. Source: Authors’ mapping of SPICT criteria on a longitudinal ageing study in India questionnaire. LASI: Longitudinal ageing study in India, SPICT-LIS: Supportive and palliative care indicator tool-low-income settings.
From the LASI data, 31,902 older adults aged 60 years and above were identified; among them, 1458 older adults with stroke and other neurological diseases were selected for estimation and further analysis. The SPICT-LIS indicators for stroke and other neurological diseases that were mapped were then compared against the older adults with stroke and other neurological diseases, and the requirement of supportive and palliative care (yes/no) was constructed as the outcome variable [Figure 2]. Subsequently, potential background characteristics that have a determinant impact on the outcome variable were identified as independent variables. It encompassed biological (age, sex and body mass index [BMI]), social (education, income, religion, caste, living status and place of residence), morbidity profile (prevalence of hypertension, diabetes, heart disease and dyslipidaemia) as well as other risk factors (habits of smoking, alcohol and physical activity status).
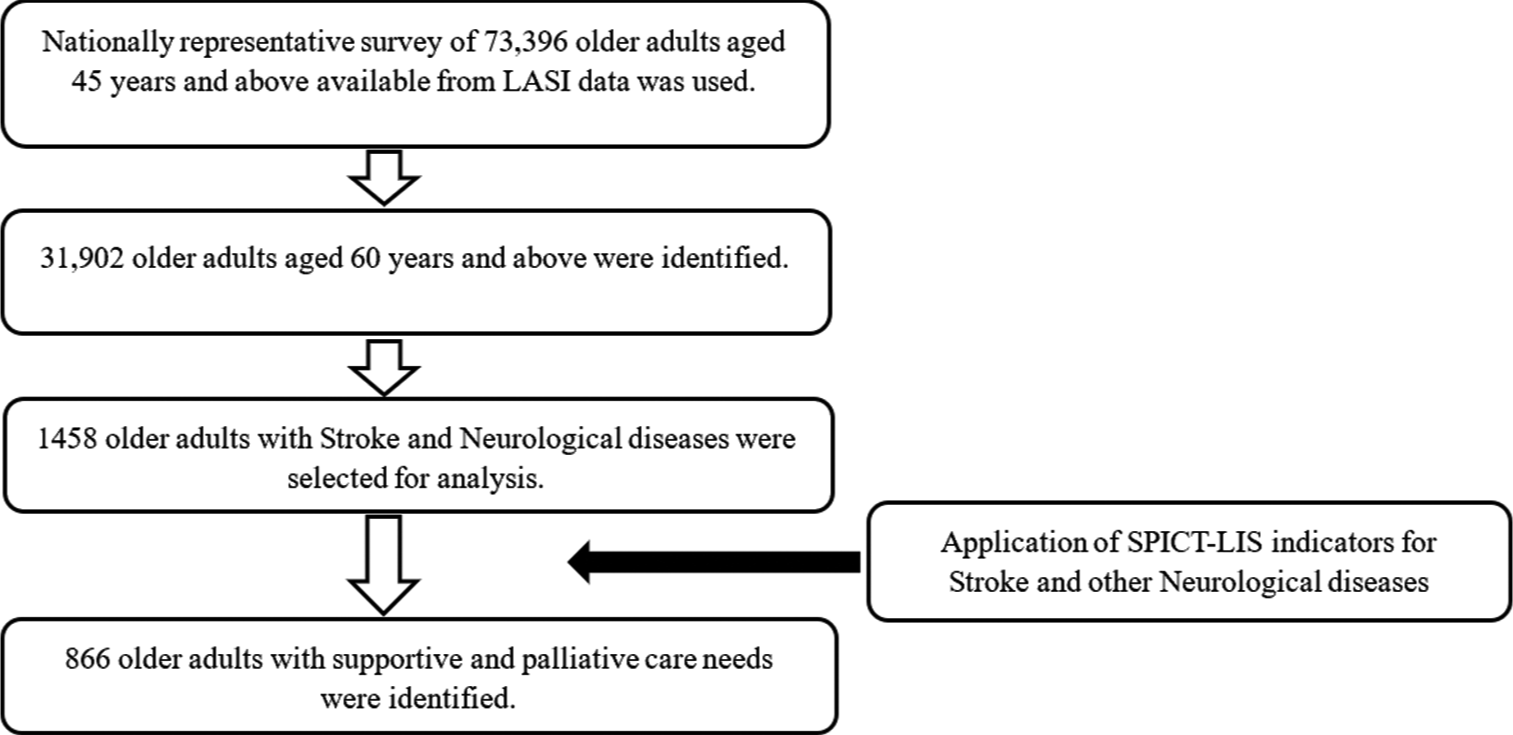
- Diagrammatic representation of study flow. Source: Author’s description of Study flow. LASI: Longitudinal ageing study in India, SPICT-LIS: Supportive and palliative care indicator tool-low-income settings.
Statistical analysis
The study used both descriptive and inferential statistics for statistical analysis. Descriptive statistics were used to estimate the supportive and palliative care needs among older adults with stroke and other neurological diseases. Since LASI followed a multistage stratified area probability cluster sampling design, survey weights were applied during the estimation process, and all the percentages provided in the tables are weighted percentages. Chi-square tests were used to confirm the disparities in these estimates among different sub-group populations. Multivariate logistic regression (odds ratio) was used for inferential statistical analysis to identify the association between the outcome variable and background characteristics. All the statistical analyses were performed using the statistical software package STATA - SE—Standard Edition 17, developed by StataCorp and located in Texas 77845, USA (StataCorp, 2021). Missing data were not included in the analysis.
RESULTS
Palliative care need among older adults with stroke and other neurological diseases
Table 1 shows that the overall prevalence of palliative and supportive care needs among older adults with stroke and other neurological diseases in India is 63.6%. In the univariate analysis, a statistically significant higher burden of palliative care needs was observed among older adults aged over 70 years (73.9%), females (67.2%), underweight (66.2%), overweight/obese (60.3%), BMI categories, older adults with primary education and below (66.5%), poorest economic category (76.5%), living alone (70.5%), low social activity (65.2%) and among older adults with hypertension (66.3%) and diabetes (63.6%) when compared against their counterparts. Furthermore, in the univariate analysis, a statistically significant lower burden of palliative care needs was observed among older adults with stroke and other neurological diseases, who engaged in vigorous (37.8%) and moderate physical activity (54.7%) compared to those who did not engage in any physical activity (67.7%).
| Description | Category | Sample n(%) | Supportive and palliative care needs | Chi-square P-value | Regression analysis for supportive and palliative care needs AOR (CI) | P-value | |
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| India | 1458 | 866 (63.6) | 592 (36.4) | ||||
| Biological profile | |||||||
| Age | ≤70 years of age | 854 (57.3) | 464 (55.8) | 390 (44.2) | 1.00® | ||
| >70 years of age | 604 (42.7) | 402 (73.9) | 202 (26.1) | 0.00 | 1.26 (0.96–1.66) | 0.10 | |
| Sex | Male | 780 (50.6) | 444 (60.0) | 336 (40) | 1.00® | ||
| Female | 678 (49.5) | 422 (67.2) | 256 (32.8) | 0.03 | 0.91 (0.65–1.25) | 0.55 | |
| BMI | Normal | 613 (53.5) | 303 (55.5) | 310 (44.5) | 1.00® | ||
| Underweight | 207 (23.8) | 123 (66.2) | 84 (33.8) | 1.49 (1.02–2.18) | 0.04 | ||
| Overweight/obese | 321 (22.7) | 186 (60.3) | 135 (39.7) | 0.01 | 1.39 (1.01–1.9) | 0.04 | |
| Social profile | |||||||
| Education | Primary education and below | 1085 (79.0) | 664 (66.5) | 421 (33.5) | 1.00® | ||
| Middle and secondary education | 239 (14.0) | 132 (52.9) | 107 (47.1) | 0.80 (0.55–1.18) | 0.27 | ||
| Higher secondary education and above | 134 (7.0) | 70 (51.6) | 64 (48.4) | 0.04 | 0.69 (0.41–1.16) | 0.16 | |
| Economic Status (Based on median per capita expenditure) | |||||||
| Poorest | 241 (19.4) | 164 (76.5) | 77 (23.5) | 1.00® | |||
| Poorer | 277 (20.2) | 172 (66.5) | 105 (33.5) | 0.77 (0.5–1.2) | 0.25 | ||
| Middle | 300 (20.8) | 178 (61.2) | 122 (38.8) | 0.71 (0.46–1.1) | 0.13 | ||
| Richer | 287 (20.3) | 167 (62.1) | 120 (37.9) | 0.60 (0.38–0.94) | 0.03 | ||
| Richest | 353 (19.3) | 185 (51.5) | 168 (48.5) | 0.01 | 0.51 (0.33–0.79) | 0.00 | |
| Religion | Hindu | 1039 (80.7) | 612 (62.8) | 427 (37.2) | 1.00® | ||
| Muslim | 197 (11.6) | 127 (68.2) | 70 (31.8) | 1.17 (0.75–1.84) | 0.48 | ||
| Other | 222 (7.7) | 127 (64.5) | 95 (35.5) | 0.26 | 0.95 (0.65–1.37) | 0.78 | |
| Caste | SC/ST | 422 (29.7) | 253 (65.4) | 169 (34.6) | 1.00® | ||
| OBC | 555 (43.8) | 314 (61.7) | 241 (38.3) | 0.81 (0.57–1.14) | 0.22 | ||
| Other | 419 (26.5) | 261 (64.3) | 158 (35.7) | 0.18 | 1.18 (0.81–1.72) | 0.40 | |
| Living status | Living alone/with others | 561 (42.2) | 371 (70.5) | 190 (29.5) | 1.00® | ||
| Living with spouse | 897 (57.8) | 495 (58.5) | 402 (41.5) | 0.00 | 0.66 (0.48–0.91) | 0.01 | |
| Residence | Urban | 582 (29.7) | 349 (63.7) | 233 (36.3) | 1.00® | ||
| Rural | 876 (70.3) | 517 (63.5) | 359 (36.5) | 0.71 | 1.07 (0.79–1.44) | 0.67 | |
| Health insurance | No | 1156 (83.6) | 679 (63.5) | 477 (36.5) | 1.00® | ||
| Yes | 294 (16.4) | 183 (63.9) | 111 (36.1) | 0.27 | 1.45 (1.06–1.99) | 0.02 | |
| Welfare schemes | Not available | 972 (67.8) | 588 (63.4) | 384 (36.6) | 1.00® | ||
| At least one available | 486 (32.2) | 278 (63.9) | 208 (36.1) | 0.22 | 0.64 (0.49–0.85) | 0.01 | |
| Social activity | Low/Nil social activity | 1270 (89) | 788 (65.2) | 482 (34.8) | 1.00® | ||
| High social activity | 188 (11.1) | 78 (50.1) | 110 (49.9) | 0.00 | 0.5 (0.34–0.74) | 0.00 | |
| Discrimination | No discrimination faced | 1393 (96.2) | 830 (63.9) | 563 (36.1) | 1.00® | ||
| At least one discrimination faced | 65 (3.8) | 36 (56.3) | 29 (43.7) | 0.50 | 0.75 (0.41–1.39) | 0.37 | |
| Experienced | No | 1237 (93.3) | 688 (61.1) | 549 (38.9) | 1.00® | ||
| Ill-treatment | Yes | 72 (6.8) | 50 (60.4) | 22 (39.6) | 0.02 | 2.34 (1.29–4.23) | 0.01 |
| Morbidity profile | |||||||
| Hypertension | No | 597 (46.4) | 332 (60.4) | 265 (39.6) | 1.00® | ||
| Yes | 861 (53.6) | 534 (66.3) | 327 (33.7) | 0.01 | 1.41 (1.06–1.87) | 0.02 | |
| Diabetes | No | 1107 (79.1) | 639 (63.6) | 468 (36.4) | 1.00® | ||
| Yes | 351 (20.9) | 227 (63.6) | 124 (36.4) | 0.02 | 1.63 (1.17–2.26) | 0.01 | |
| Dyslipidaemia | No | 1339 (94.3) | 787 (64.0) | 552 (36.0) | 1.00® | ||
| Yes | 119 (5.7) | 79 (55.9) | 40 (44.1) | 0.10 | 1.53 (0.93–2.54) | 0.10 | |
| Heart disease | No | 1304 (89.8) | 777 (64.1) | 527 (35.9) | 1.00® | ||
| Yes | 154 (10.2) | 89 (58.8) | 65 (41.2) | 0.66 | 1.07 (0.7–1.64) | 0.74 | |
| Feeling depressed | No | 893 (63.9) | 490 (58.1) | 403 (41.9) | 1.00® | ||
| Yes | 426 (36.2) | 253 (65.8) | 173 (34.2) | 0.12 | 1.14 (0.86–1.51) | 0.38 | |
| Risk factors profile | |||||||
| Tobacco use | No | 862 (55.9) | 524 (64.7) | 338 (35.3) | 1.00® | ||
| Yes | 591 (44.1) | 339 (62.0) | 252 (38.0) | 0.19 | 1.05 (0.78–1.43) | 0.74 | |
| Alcohol use | No | 1162 (84.2) | 701 (64.8) | 461 (35.2) | 1.00® | ||
| Yes | 291 (15.8) | 162 (56.2) | 129 (43.8) | 0.14 | 0.91 (0.64–1.31) | 0.63 | |
| Physical activity | No physical activity | 1240 (84.1) | 783 (67.7) | 457 (32.3) | 1.00® | ||
| Only vigorous | 91 (6.9) | 27 (37.8) | 64 (62.2) | 0.34 (0.2–0.58) | 0.00 | ||
| Only moderate | 98 (6.9) | 49 (54.7) | 49 (45.3) | 0.77 (0.46–1.29) | 0.32 | ||
| Both vigorous and moderate | 21 (2.2) | 1 (5.8) | 20 (94.2) | 0.00 | 0.03 (0.003–0.29) | 0.01 |
Source: Authors’ estimation using LASI data. AOR: Adjusted odds ratio, CI: 95% Confidence interval, BMI: Body mass index, ®Reference category
In the multivariate logistic regression analysis of older adults with stroke and other neurological diseases, a higher burden of palliative care need was observed among those who belonged to underweight (Adjusted odds ratio [AOR] = 1.49) and overweight/obese BMI categories (AOR = 1.39) when compared with normal weight category and among those who experienced ill-treatment (AOR = 2.34) when compared with those who did not experience ill-treatment. Among the variables in the morbidity profile, a higher burden of palliative care needs was observed among those with hypertension (AOR = 1.41) and diabetes (AOR = 1.63) than their counterparts. Interestingly, older adults with health insurance had a higher burden of palliative care needs (AOR = 1.45) when compared with older adults without health insurance.
Furthermore, in the regression analysis of older adults with stroke and other neurological diseases, a significantly lower burden of palliative care needs was observed among the older adults in the richer (AOR = 0.60) and richest (AOR = 0.51) economic groups when compared with those in the poorest economic group. Older adults who live with their spouse had a lower burden of palliative care needs (AOR = 0.66) when compared with those who live alone or live with others. Similarly, older adults receiving at least one social support scheme had a lower burden of palliative care needs (AOR = 0.64) when compared with those without any social support scheme and older adults with high social activity also had lower palliative care needs (AOR = 0.50) when compared against those with low or no social activity. In the analysis of physical activity, older adults with stroke and other neurological diseases who engaged only in vigorous physical activity and both moderate and vigorous physical activity had a lower burden of palliative care needs (AOR = 0.34 and AOR = 0.03, respectively) when compared with older adults with no physical activity.
DISCUSSION
In the current analysis of LASI data, 63.5% of older adults with stroke and neurological diseases were identified to have supportive and palliative care needs using SPICT-LIS criteria. Although the tool specifies ‘supportive and palliative care’ in its nomenclature, in practice, both these terms are used interchangeably.[23] The WHO defines palliative care as ‘Palliative care is an approach that improves the quality of life of patients (adults and children) and their families who are facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and correct assessment and treatment of pain and other problems, whether physical, psychosocial or spiritual.[8]’ The National Cancer Institute defines supportive care as ‘care given to improve the quality of life of people who have an illness or disease by preventing or treating, as early as possible, the symptoms of the disease and the side effects caused by treatment of the disease. Supportive care includes physical, psychological, social and spiritual support for patients and their families.[24] These definitions show that the goal of supportive care and palliative is to improve the quality of life, and they also follow similar processes to achieve this goal.
In stroke and other neurological diseases, there is a significant loss of function, increased dependence and cognitive impairment in comparison with other chronic diseases, and these reasons contribute to high supportive and palliative care needs in these patients.[25] In the sub-group analysis, several variables in the biological profile, social profile and risk factor profile were found to be associated with supportive and palliative care needs. In the trajectory of neurological diseases, the demand for supportive and palliative care needs increases with advancing disease and age. [25,26] In this current study, 74% of those more than 70 years of age with stroke and other neurological diseases required palliative care. The changes associated with advancing age, such as increasing frailty, cognitive impairment and declining functional status along with progressive neurological disease, cause and accelerate these impairments, resulting in a higher burden of palliative care needs in these individuals.
In the present study, both the underweight and overweight/obese categories had a higher burden of palliative care needs. This was observed in both univariate and multivariate analysis. Studies show that older adults who are underweight have lower life expectancy and lower functional status when compared with older adults who have normal weight,[27] and malnutrition also plays a role in the development of geriatric syndromes.[28] Furthermore, being underweight is an indicator of poor and deteriorating health in the supportive and palliative care indicator tool general criteria. With regard to overweight/obese individuals, the presence of multiple morbidities, functional impairment, malnutrition and accelerated decline in health status could be the possible explanation for higher palliative needs among them.[29] Although the palliative and supportive care need is high in this population, it is essential to note that the actual utilisation of palliative care services is less among obese individuals when compared with normal-weight individuals, and this poor utilisation among obese individuals is associated with adverse outcomes such as higher expenditure and institutional deaths.[30]
In the current study, 6.8% of older adults with stroke and other neurological diseases reported experiencing ill treatment. In the regression analysis, higher palliative care need was observed among the older adults who reported experiencing ill-treatment. Elder abuse is not just a social problem but also a public health problem. Increased vulnerability, dependence and caregiver stress in the context of life-limiting illnesses are crucial factors in abuse.[31,32] As palliative care seeks not only to improve the quality of life of patients with life-limiting illnesses but also to address caregiver burden, anxiety and stress, it can play a major role in addressing this problem.[33,34] Among the morbidity profiles, the presence of hypertension and diabetes was found to be associated with higher supportive and palliative care needs in the regression analysis. Hypertension is known to cause end-organ damage, resulting in stroke, heart failure, renal failure and vascular diseases;[35] Similarly, the complications of diabetes follow a similar disease trajectory.[36] Both hypertension and diabetes are prevalent comorbidities with other chronic conditions and a significant predictor of stroke and may be the reason for their association with supportive and palliative care needs.[37]
The economic category of older adults with stroke and neurological diseases emerged as a significant factor associated with supportive and palliative care needs. The burden of palliative care needs among the richest economic quintile was 51.5%, but among the poorest economic quintile, it was 76.5%. A similar trend was also confirmed in the multivariate analysis. In a study conducted among individuals with palliative care needs in five Asian countries, including India, where individuals from lower socioeconomic categories were observed to experience greater suffering in several domains.[38] The WHO also estimates that 76% of those who need palliative care live in low-middle-income countries, and the highest proportion of need is among low-income countries.[8] These findings suggest that palliative care needs are strongly influenced by economic status.
In the current study, the burden of supportive and palliative care needs was observed to be lower among older adults with stroke and neurological diseases who received support from social welfare schemes and whose social activity levels were high. Several studies show that social support for older adults with palliative care needs produces a better quality of life, health status, satisfaction and mental well-being. [39-43] Like social support, studies also show that social activity among older adults reduces mortality and institutionalisation and improves the health status of older adults. These reasons could explain the lower burden of palliative care needs among them. Furthermore, among older adults with stroke and other neurological diseases, the burden of palliative care needs was observed to be lower among those who engage in vigorous physical activity or both moderate and vigorous physical activity. Among those with stroke or other neurological diseases, physical activity and physical rehabilitation play a significant role in preserving and improving functional ability. [44,45] These findings underscore the importance of improving awareness and access to physical rehabilitation services for older adults affected by stroke and other neurological diseases.
Strengths and limitations
This is the first study to estimate supportive and palliative care needs in India using a nationally representative sample. SPICT-LIS, a validated instrument in identifying individuals with supportive and palliative care needs, is another merit of this current study. Since the study used a nationally representative sample of the older Indian population, the results have good external validity. Nevertheless, the non-availability of an indicator considered for palliative care needs by SPICT-LIS, like episodes of aspiration pneumonia, breathlessness or respiratory failure in the LASI data, maybe a limitation of this study. The actual palliative estimation, therefore, may be slightly higher than the present estimation. The limitations of the LASI survey apply to the current paper. These include respondent fatigue because of lengthy surveys and local dialect challenges during survey administration.
CONCLUSION
The supportive and palliative care needs among the older population with stroke and other neurological diseases in India are high. The findings of this study underscore the importance of screening for supportive and palliative care needs among patients with stroke and other neurological diseases to identify these unmet needs. The palliative care needs in this group are influenced by their BMI status, economic category, the experience of ill-treatment, comorbid conditions, social support, social engagement and physical activity. As the proportion of older adults is estimated to double in the next three decades in India, the workforce trained in the provision of generalist and specialist palliative care will be required to meet the growing supportive and palliative care needs of the country.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Geriatric Palliative Care: A View of Its Concept, Challenges and Strategies. BMC Geriatr. 2018;18:220.
- [CrossRef] [PubMed] [Google Scholar]
- United Nations: Department of Economic and Social Affairs: Population Division. In: World Population Ageing 2019. New York: United Nations; 2021.
- [Google Scholar]
- Aging and Health. 2022. Factsheet. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-andhealth#:~:text=at%20this%20time%20the%20share,2050%20to%20reach%20426%20million [Last accessed on 2023 Dec 01]
- [Google Scholar]
- Development of Physical Disability in Older Adults. CAS. 2011;4:184-91.
- [CrossRef] [PubMed] [Google Scholar]
- Morbidity Profile and Its Relationship with Disability and Psychological Distress among Elderly People in Northern India. Int J Epidemiol. 2003;32:978-87.
- [CrossRef] [PubMed] [Google Scholar]
- Mental Health of Older Adults. 2023. Factsheet. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults [Last accessed on 2024 Jan 13]
- [Google Scholar]
- The Escalating Global Burden of Serious Health-related Suffering: Projections to 2060 by World Regions, Age Groups, and Health Conditions. Lancet Global Health. 2019;7:e883-92.
- [CrossRef] [PubMed] [Google Scholar]
- Global Atlas of Palliative Care. 2020. Available from: https://cdn.who.int/media/docs/default-source/integrated-health-services-(ihs)/csy/palliative-care/whpca_global_atlas_p5_digital_final.pdf?sfvrsn=1b54423a_3 [Last accessed on 2024 Jan 13]
- [Google Scholar]
- Demographics of Population Ageing in India In: Giridhar G, Sathyanarayana KM, Kumar S, James KS, Alam M, eds. Population Ageing in India. Cambridge, UK: Cambridge University Press; 2014. p. :1-41. Available from: https://www.cambridge.org/core/product/identifier/cbo9781139683456a014/type/book/part [Last accessed on 2024 Jan 03]
- [Google Scholar]
- Palliative Care Need in India: A Systematic Review and Meta-analysis. Indian J Palliat Care. 2023;29:375-87.
- [CrossRef] [PubMed] [Google Scholar]
- India Ageing Report 2023 Caring for Our Elders: Institutional Responses New Delhi: International Institute for Population Sciences and United Nations Population Fund; 2023.
- [Google Scholar]
- Illness-related Suffering and Need for Palliative Care in Rohingya Refugees and Caregivers in Bangladesh: A Cross-sectional Study. PLoS Med. 2020;17:e1003011.
- [CrossRef] [PubMed] [Google Scholar]
- Barriers to Access to Palliative Care. Palliat Care. 2017;10:1-6.
- [CrossRef] [PubMed] [Google Scholar]
- Estimating the Need for Palliative Care in an Urban Resettlement Colony of New Delhi, North India. Indian J Palliat Care. 2022;28:434-8.
- [CrossRef] [PubMed] [Google Scholar]
- Estimation of Need for Palliative Care among Noncancer Patients Attending a Tertiary Care Hospital. Indian J Palliat Care. 2017;23:403-8.
- [CrossRef] [PubMed] [Google Scholar]
- Estimation of Palliative Care Need in the Urban Community of Puducherry. Indian J Palliat Care. 2017;23:81-7.
- [CrossRef] [PubMed] [Google Scholar]
- Screening for Palliative Care Needs in the Community Using SPICT. Med J Armed Forces India. 2023;79:213-9.
- [CrossRef] [PubMed] [Google Scholar]
- Ageing as a Risk Factor for Neurodegenerative Disease. Nat Rev Neurol. 2019;15:565-81.
- [CrossRef] [PubMed] [Google Scholar]
- Development and Evaluation of the Supportive and Palliative Care Indicators Tool (SPICT): A Mixed-methods Study. BMJ Support Palliat Care. 2014;4:285-90.
- [CrossRef] [PubMed] [Google Scholar]
- Systematic Adaptation of the Thai Version of the Supportive and Palliative Care Indicators Tool for Low-income Setting (SPICT-LIS) BMC Palliat Care. 2021;20:35.
- [CrossRef] [PubMed] [Google Scholar]
- Longitudinal Ageing Study in India (LASI) Wave 1, 2017-18, India Report. In: Mumbai: International Institute for Population Sciences (IIPS), National Programme for Health Care of Elderly (NPHCE), MoHFW, Harvard T. H. Chan School of Public Health (HSPH) and the University of Southern California (USC) 2020. 2020.
- [Google Scholar]
- The Terms Supportive and Palliative Care-analysis of Their Prevalence and Use: Quasi-systematic Review. Palliat Med Pract. 2021;15:248-53.
- [Google Scholar]
- NCI Dictionary of Cancer Terms. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/supportive-care [Last accessed on 2024 Jul 18]
- [Google Scholar]
- Palliative Care in Neurology. Mayo Clin Proc. 2017;92:1592-601.
- [CrossRef] [PubMed] [Google Scholar]
- Palliative Care for Frail Older People. Clin Med (Lond). 2014;14:292-5.
- [CrossRef] [PubMed] [Google Scholar]
- The Role of Underweight in Active Life Expectancy among Older Adults in Japan. J Gerontol B Psychol Sci Soc Sci. 2021;76:756-65.
- [CrossRef] [PubMed] [Google Scholar]
- Malnutrition in Older Adults-Recent Advances and Remaining Challenges. Nutrients. 2021;13:2764.
- [CrossRef] [PubMed] [Google Scholar]
- The Relationship of Obesity to Hospice Use and Expenditures: A Cohort Study. Ann Intern Med. 2017;166:381-9.
- [CrossRef] [PubMed] [Google Scholar]
- Domestic Abuse in the Context of Life-Limiting Illness: A Systematic Scoping Review. Health Soc Care Community. 2023;2023:1-24.
- [CrossRef] [Google Scholar]
- Elder Neglect and Abuse. A Primer for Primary Care Physicians. Geriatrics. 2003;58:37-40, 42-4
- [Google Scholar]
- Family Caregiver Mistreatment of the Elderly: Prevalence of Risk and Associated Factors. BMC Public Health. 2018;18:167.
- [CrossRef] [PubMed] [Google Scholar]
- Elder Abuse and Palliative Care: The Time to Act is Now! New Delhi: Indian Association of Palliative Care; 2022. p. :5.
- [Google Scholar]
- End Organ Damage in Hypertension. Deutsches Ärzteblatt International 2010 Available from: https://www.aerzteblatt.de/10.3238/arztebl.2010.0866 [Last accessed on 2023 Dec 27]
- [CrossRef] [PubMed] [Google Scholar]
- A Longitudinal Clinical Trajectory Analysis Examining the Accumulation of Co-morbidity in People with Type 2 Diabetes (T2D) Compared with Non-T2D Individuals. Diabetes Ther. 2023;14:1903-13.
- [CrossRef] [PubMed] [Google Scholar]
- Risk-factor Clustering and Cardiovascular Disease Risk in Hypertensive Patients. Am J Hypertens. 2007;20:599-607.
- [CrossRef] [PubMed] [Google Scholar]
- Socioeconomic Inequalities in Suffering at the End of Life among Advanced Cancer Patients: Results from the APPROACH Study in Five Asian Countries. Int J Equity Health. 2020;19:158.
- [CrossRef] [PubMed] [Google Scholar]
- Social Support and Self-reported Health Status of Older Adults in the United States. Am J Public Health. 2009;99:1872-8.
- [CrossRef] [PubMed] [Google Scholar]
- The Impact of Social Support on the Quality of Life among Older Adults in China: An Empirical Study Based on the 2020 CFPS. Front Public Health. 2022;10:914707.
- [CrossRef] [PubMed] [Google Scholar]
- Association of Social Support with Functional Outcomes in Older Adults Who Live Alone. JAMA Intern Med. 2022;182:26-32.
- [CrossRef] [PubMed] [Google Scholar]
- Psychosocial Care in Cancer. Curr Psychiatry Rep. 2012;14:23-9.
- [CrossRef] [PubMed] [Google Scholar]
- Social Support and Quality of Life in Cancer Patients: A Study of Palliative Shelters in West Java. Matrix Sci Med. 2022;6:40.
- [CrossRef] [Google Scholar]
- A Comprehensive Review of Physical Therapy Interventions for Stroke Rehabilitation: Impairment-Based Approaches and Functional Goals. Brain Sci. 2023;13:717.
- [CrossRef] [PubMed] [Google Scholar]
- Physical Activity in Neurological Disorders: A Narrative Review. Eur J Ther. 2023;29:97-102.
- [CrossRef] [Google Scholar]




