
Translate this page into:
Telemedicine as an Acceptable Model of Care in Advanced stage Cancer Patients in the Era of Coronavirus Disease 2019 – An Observational Study in a Tertiary Care Centre

*Corresponding author: Sushma Bhatnagar, Deapartment of Onco-anaesthesia and Palliative Medicine, All India Institute of Medical Sciences, New Delhi, India. shumob@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Adhikari SD, Biswas S, Mishra S, Kumar V, Bharti SJ, Gupta N, et al. Telemedicine as an acceptable model of care in advanced stage cancer patients in the era of coronavirus disease 2019 – An observational study in a tertiary care centre. Indian J Palliat Care 2021;27(2):306-12.
Abstract
Objectives:
The availability of routine care for patients with cancer during the coronavirus disease 2019 (COVID-19) pandemic has become challenging, and the use of telemedicine can be promising in this area. The objective of the study is to evaluate the feasibility of telemedicine-based palliative interventions in cancer patients.
Materials and Methods:
This retrospective study was conducted in a tertiary care centre with 547 follow-up patients who used palliative medicine teleconsultation services. The following data were retrieved from the records: Patient’s reason for the call, the main barriers to a hospital visit, the assistance given to them by the physician on the call and the patients’ satisfaction with the service on a 4-point scale. The data were analysed using percentages for categorical variables and mean/standard deviation for quantitative variables.
Results:
Out of the 547 patients, 462 (84.46%) utilised voice calling service, and the major reason for not visiting the hospital were cited to be fear of contracting COVID-19 (37.3%), inability to attend due to health constraints (7.13%) and issues with transportation (48.8%). The majority of the calls (63.62%) calls were regarding uncontrolled symptoms of the primary diseases. A total of 402 (73.49%) patients were very satisfied, and a total of 399 (72.94%) decided to continue to use this medium in the future as well.
Conclusion:
Telemedicine is a good modality for the assessment of chronic pain and providing symptomatic supportive care in patients with cancer in the COIVD-19 pandemic.
Keywords
Cancer
Coronavirus disease 2019
Palliative medicine
Patient satisfaction
Telemedicine

INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic has turned out to be a catastrophic health scare that has left the health systems all over the world in shambles. It has become particularly difficult to provide routine care to patients with chronic medical conditions such as malignancies. The lockdown in the country, restricted movement, coupled with the shunting of resources (including manpower), and risk of infection, has forced hospitals to limit the inflow of patients to the hospital. In cancer patients, who often have physical or cognitive impairments, such restrictions affect them disproportionately.[1,2] Teleconsultation has been described as a tool to effectively manage patients during this pandemic. Although teleconsultation has been described as early as 1879, modern telemedicine has developed and evolved in the late 20th century.[3-6] Telemedicine has also been used in modern oncology as a tool to deliver supportive care with reports showing high satisfaction in patients.[7] Although, India has a very high burden of cancer patients who are dependent on tertiary care centres for routine care, the concept of telemedicine is relatively new, and rural areas may be neglected in this field. As the catchment area of hospitals is large, many patients travel long distances for their regular visits. Hence, implementing teleconsultation may be needed to ensure continuity of care. The aim of this study was to, therefore, assess the feasibility of telemedicine as a tool for palliative medicine.
MATERIALS AND METHODS
This retrospective study was done to analyse the telemedicine service from 25 March 2020 to 30 June 2020 at the palliative medicine unit of a tertiary care cancer centre in North India. The study was conducted after the institute’s ethics committee approval (IEC/841/7/2020). All patients who availed of the teleconsultation services during the study period were recruited. The unregistered patients who were referred from other departments and had no prior physical visit and patients or attendants who were not well-versed in English and Hindi language were excluded from the study. The department had a voice call-based telemedicine service already in place for the consultation of follow-up patients. In the light of the current pandemic, anticipating a need for detailed interaction with the patients, a smartphone-based 24/7 model for conducting audio-visual consultations was created following the Telemedicine Practice Guidelines of India.[8] Phone calls, text messages and smartphone-based applications, such as WhatsApp Messenger and Skype for audio-visual consultation, were used. All the patients registered with the department were provided with a phone number for consultations and follow-up. A trained palliative medicine physician was available round the clock for consultations. On receiving a consult on the phone, the practitioner would access the electronic record of the patients and provide appropriate medical advice. The patients were also provided with the contact numbers of palliative medicine centres in other parts of India to procure opioids if they cannot visit our hospital. Multidisciplinary assistance was provided to the patients by providing the contact details of the telemedicine service of the other specialities if needed. The details of demographics, clinical features, diagnosis, the reason for teleconsultation, main barriers to a hospital visit, the advice is given, and patient satisfaction were entered into a case reporting form. Each caller at the end of the call was asked to measure his/her satisfaction with the service on a 4-point scale: Very satisfied (4), satisfied (3), partially satisfied (2) and unsatisfied (1). The data from the case record form were tabulated using a spreadsheet. Quantitative data were represented with mean and standard deviation, and the categorical data were represented with numbers and percentages. Mann–Whitney U-test was used to calculate the difference between satisfaction scores.
RESULTS
A total of 547 patients were recruited. Among the patients who availed of our teleconsultation service, a total of 233 (42.6%) patients belonged to the same state in which the hospital is located while the other 314 (57.4%) patients resided in the neighbouring states. A total of 15 patients (2.74%) belonged to the paediatric age group. The rest of the patients were adults. The median age was 45 years, with a range of 5–83 years. The disease characteristics, duration of the disease and status of the disease at the time of teleconsultation are summarised [Table 1].
| Patient demographics | Number of patients (%) Total = 547 | |
|---|---|---|
| Age | >18 years | 532 (97.26) |
| <18 years | 15 (2.74) | |
| Sex | Males | 263 (48) |
| Females | 284 (52) | |
| Residence | Delhi NCR | 233 (42.56) |
| Outside NCR | 314 (57.40) | |
| Educational qualification of person attending call | Illiterate | 12 (2.19) |
| Upto 5th standard | 27 (4.94) | |
| Upto 12th standard | 275 (50.27) | |
| Graduate and above | 233 (42.6) | |
| Telecommunication Characteristics | Number of patients (%) Total = 547 | |
| Type of calls | Voice | 462 (84.46) |
| Video | 79 (14.44) | |
| Text | 4 (0.73) | |
| Number of Calls | Single | 420(76.78) |
| Multiple | 127(23.21) | |
| Duration of Calls (minutes) | <5 | 46(8.41) |
| 5-10 | 264(48.26) | |
| 10-15 | 203(37.11) | |
| >15 | 34(6.22) | |
| Timing of calls | 6am – 10am | 66 (12.07) |
| 10am – 2pm | 327 (59.79) | |
| 2pm – 8pm | 115 (21.02) | |
| 8pm – 6am | 39 (7.13) | |
| Distribution of Malignancies | ||
| Disease Characteristics | Variables | Number of patients (%) Total = 547 |
| Duration of disease | <6months | 192(35.1) |
| 6months – 1 year | 239(43.7) | |
| >1 year | 116(21.2) | |
| Status of Disease | Under Evaluation | 54 (9.87) |
| Ongoing Treatment with Curative Intent | 288 (52.54) | |
| Cancer Survivor | 204 (37.3) | |
| Cancer Survivor | 4 (0.73) | |
| Type of Malignancy | Lung malignancy | 50 (9.14) |
| Gastrointestinal Malignancy | 64 (11.7) | |
| Hepatobiliary Malignancy | 56 (10.23) | |
| Gynaecological Malignancy | 45 (8.22) | |
| Bone and Soft Tissue Malignancy | 69 (12.61) | |
| Urogenital Malignancy | 31 (5.66) | |
| Breast Malignancy | 92 (16.82) | |
| Head and Neck Malignancy | 91 (16.64) | |
| Haematological Malignancy | 28 (5.18) | |
| Neuroendocrine Tumours | 14 (1.83) | |
| Carcinoma of Unknown Primary | 7 (1.28) | |
The major reasons restricting the outpatient department (OPD) visits are summarised [Figure 1]. The major reasons for the utilisation of teleconsultation have been summarised [Figure 2]. Out of the total of 547 patients, 282 had a chief complaint of pain and 45 shortness of breath, 31 complained of nausea and/or vomiting, 22 had abdominal distension, 20 patients complained of features of mucositis, 13 had dysphagia and 7 complained of bleeding amongst other complaints. This was an open-ended question. Most complaints were resolved with a single-time call (420); however, multiple calls were made by 127 patients [Table 1]. The majority of the patients utilised the voice calling service (462,84.46%). Three terminally ill patients were given endof-life care over video calls after thorough verbal consent. One call was made by the son of an expired patient who was concerned regarding the procedure to return the opioids. Of the advice given to the patients on teleconsultation, change of dosage or formulation or prescription of new medication was the most common (n = 266). A total of 132 patients were advised in-person visits, either for examination or for prescription of opioids (n = 32, 5.85%). Telecounselling regarding disease and further treatment course was required in 10 cases, home-based management in 47 cases and house visit by a palliative care team was arranged in 11 cases. Eight patients required emergency hospital evaluation and management, whereas, six patients were asked to visit the nearest hospital with the palliative medicine department in their state for assessment [Figure 3].
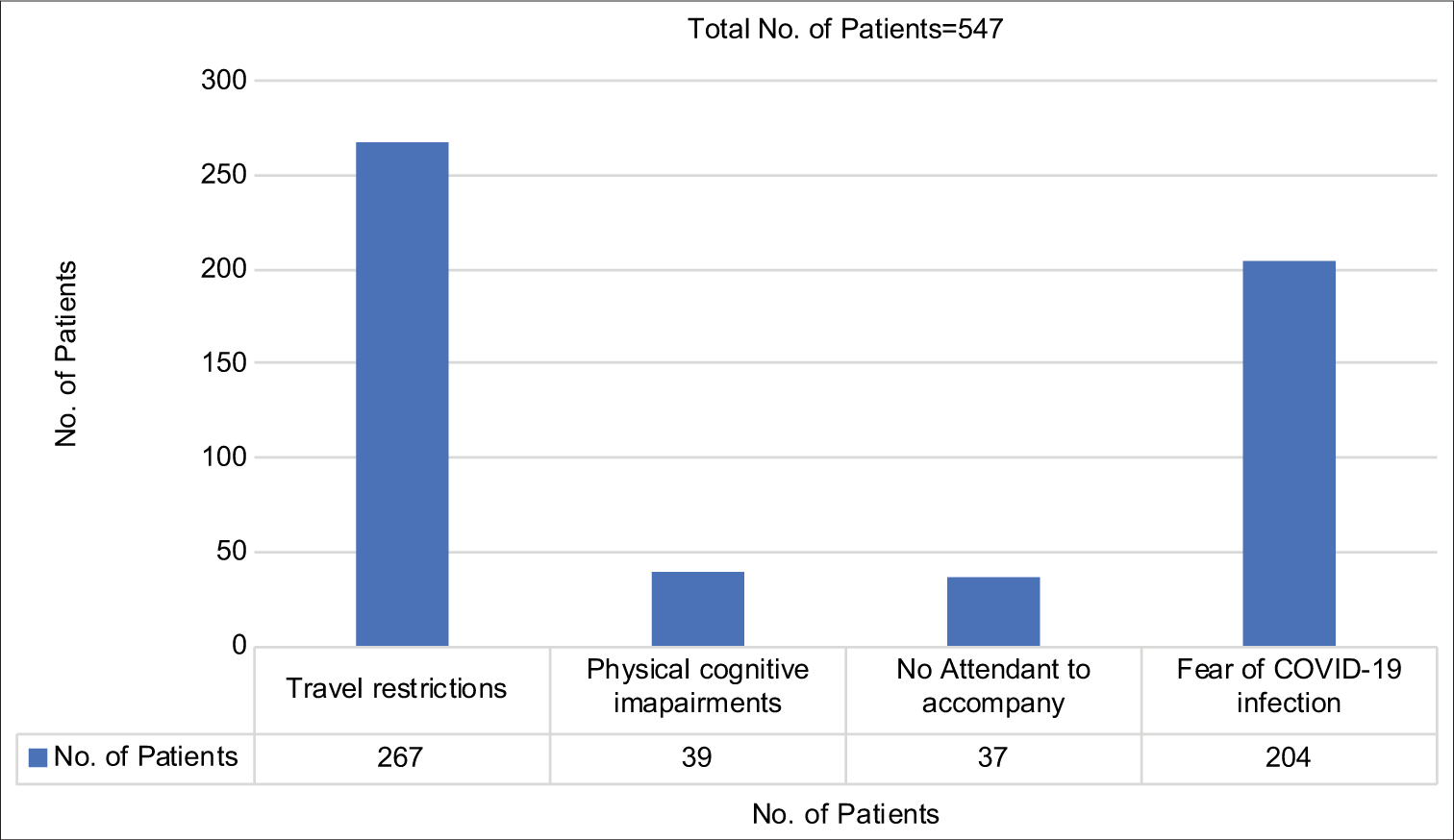
- Reasons cited for utilising telemedicine.
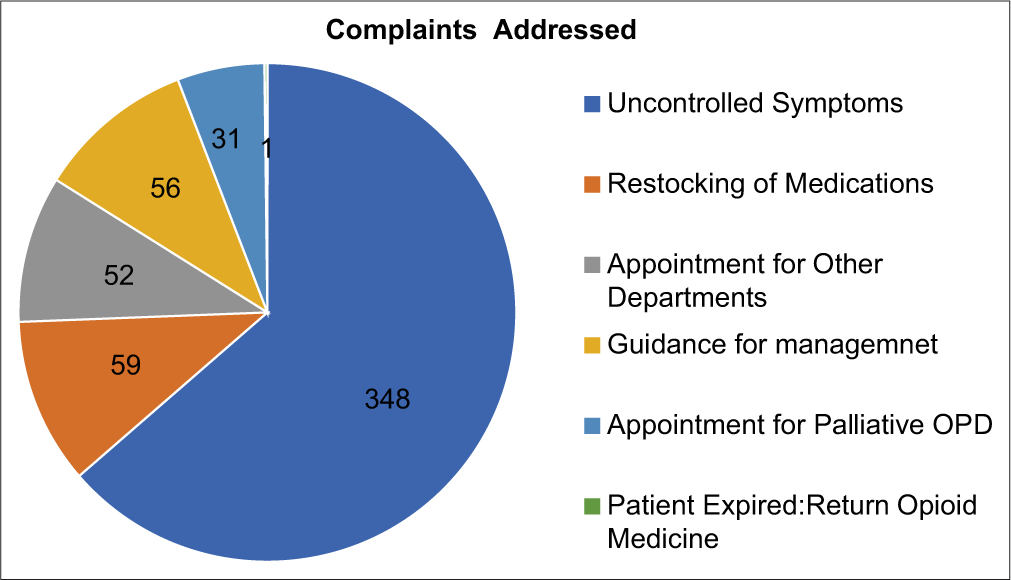
- Chief complaints of the patients addressed using teleconsultation.
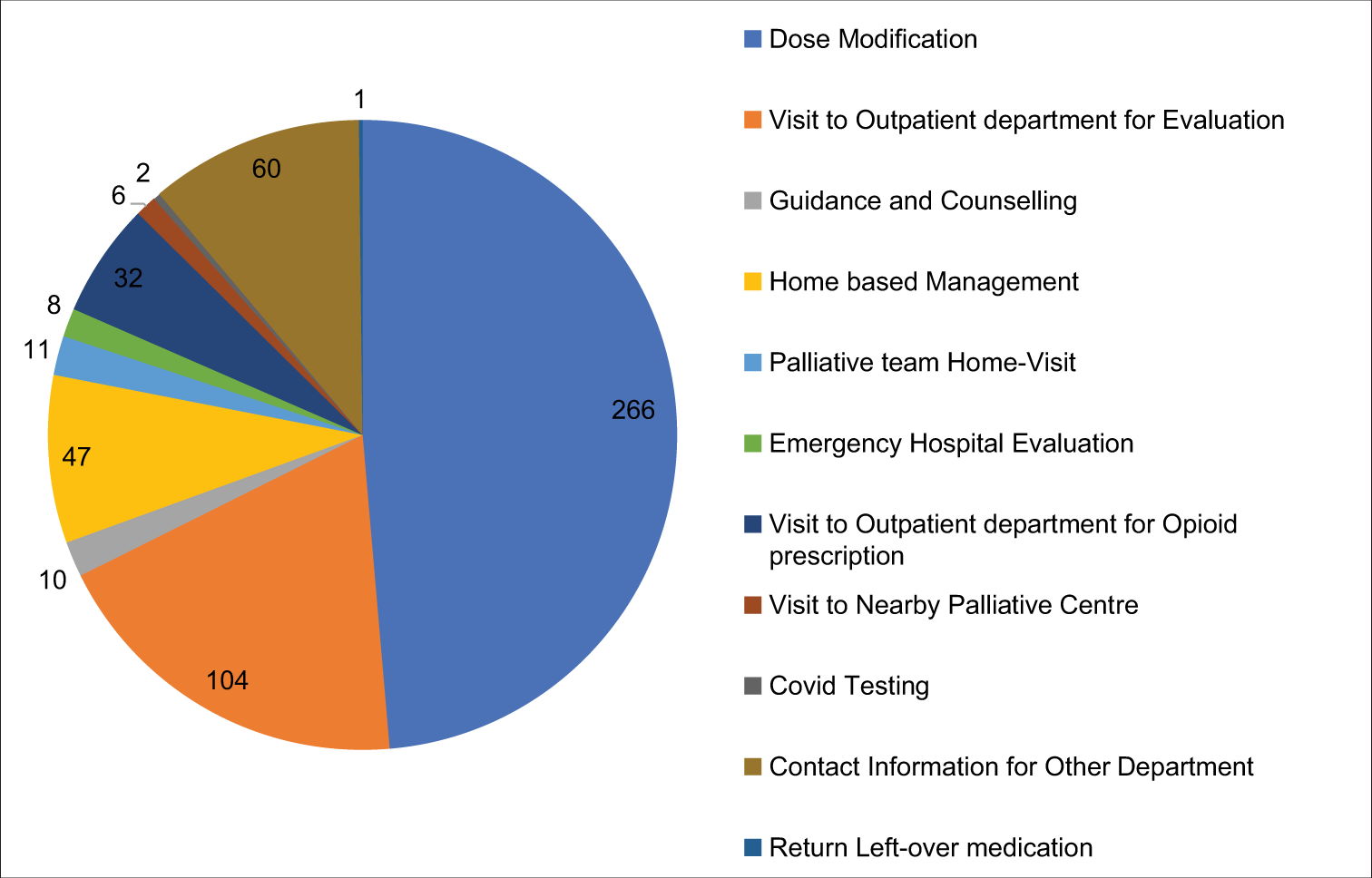
- Final advice given to the patients on teleconsultation.
On satisfaction survey of the 547 consults, a total of 73.9% of the patients were very satisfied, and 2.65% were unsatisfied. The 4-point Likert scale is depicted in Figure 4. When the median satisfaction score was computed using the Mann–Whitney U-test between individuals who consulted once (n = 420) and individuals who consulted more than once (n = 127), the difference was not significant (P = 0.328).
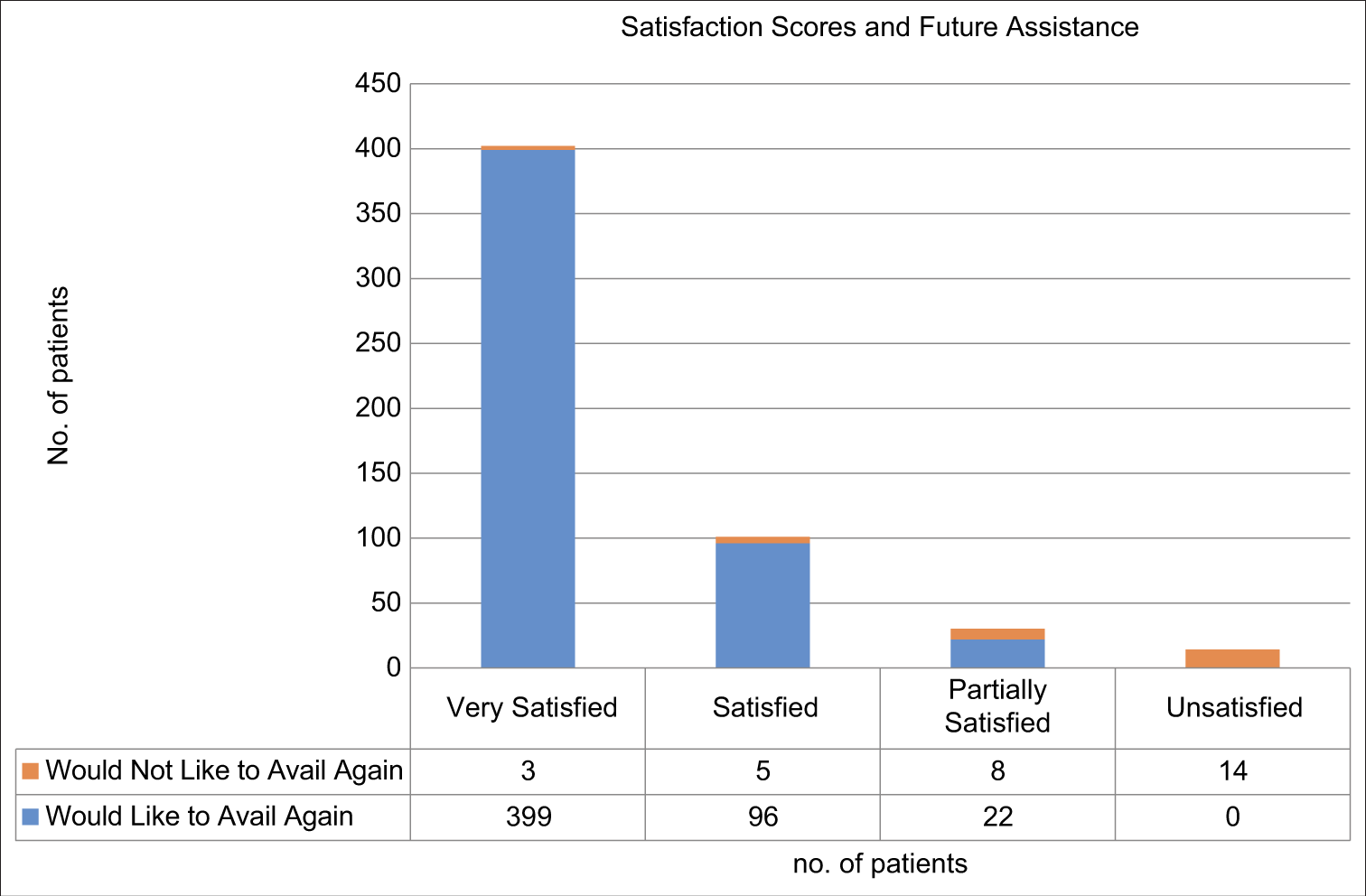
- Satisfaction score (4-point Likert scale) shows high satisfaction levels with telemedicine use.
DISCUSSION
Telemedicine plays an important role in decreasing COVID-19 transmission by avoiding close contact. It is useful for follow-up, prognostication and evaluation of treatment response. Our previous positive experience with telemedicine had encouraged us to implement this service with improved technology which included video calling with WhatsApp and Skype mobile applications.[9,10] This telemedicine platform enabled the use of popular technology to communicate between the patients and the palliative care team. WhatsApp was chosen as it is the leading social media platform for communication in India with more than 340 million users.[11] Around 20% of patients were not acquainted with its use or did not have the app on their phones. However, their relatives and friends could assist and thus attend the video conferencing.
The enhanced teleconsultation services reduced the outpatient footfalls for our palliative medicine department dramatically by 60% (1232 in February 2020 and 497 in June 2020). Another study from our institution showed a drop in single-day average footfall during the pandemic with regard to outpatient, inpatient and consultation from another department; and the number of teleconsultation calls from 2019.[9] Some studies have shown that the use of voice calls has to lead to a reduction in the number of inpatient admissions. In a study where telephonic and video consultations were done by the nurse round the clock, a total of 98.5% of calls resulted in patients staying at their homes.[12] In their survey, 46% had cancer, and 42% had a non-cancer diagnosis for palliative care. In another survey, there was a reduction of 51% in OPD visits following the implementation of teleconsultation during the COVID-19 pandemic in India.[13] There was a small-to-moderate reduction in pain, disability and distress in patients with chronic pain availing teleconsultation in comparison to patients who received standard of care as described in two systematic reviews.[14,15] According to an Expert Group from China and other study groups, telemedicine may have an important role in providing care to patients with chronic illnesses by decreasing the risk of acquiring COVID infection during physical visits.[6,16]
Most of the attendants calling were either educated up to 12th standard or were graduates and above. Even though this made communication easier, most attendants calling had a clear understanding of what instructions were given. Whenever there were problems in communication, prescriptions were typed out in detail in messages. At the end of each call, the caller was asked to repeat the prescription to their understanding to ensure correction information was received.
In our study, most of the patients utilised voice calling service, and 14% of the patients availed themselves of video calls to communicate. Video calls helped in the inspection of the patient. In the ‘Gold Line’ service assessment, 1813 individuals were aided via 4533 telephone calls and 573 video consultations.[12] In a 2015 Cochrane systematic review, video calls were compared with voice calls or physical visits in patients with chronic diseases. The outcomes were found to be similar in both groups.[17] Around 76% of consults were resolved in a single call; however, on the other extreme, two patients were required to call 6 times to satisfactorily understand the modification of medications. This was attributed to poor internet quality in one case and the hearing disability of the patient in another. Most calls were received between 10 am and 2 pm (59.79%) and 2 pm–8 pm (21.02%). Such survey data can help us maximise our output by increasing the number of telephone lines and physicians available at the time of maximum requirement.
Our survey showed that 63.62% of consults were regarding uncontrolled symptoms related to the primary disease, and out of these 282 patients had a chief complaint of pain and 45 shortness of breath. Breathlessness was assessed using the modified Medical Research Council dyspnoea scale. Grades 0–1 were managed at home whereas in those with Grades 2–4, a chest X-ray was advised in addition to general home-based management depending on the diagnosis. Abdominal X-ray or ultrasonography was advised for persistent abdominal distension, vomiting or constipation which were unresolved despite multiple consultations. They were also advised to visit the OPD or emergency department of any hospital nearby.
Unfortunately, we could not follow up with all the patients except for those who visited the OPD. Two hundred and sixty-six patients were advised to modify the medications they were already prescribed, including analgesics. However, 132 patients required in-person visits, either for examination or for prescription of opioids. This included 15 patients with dyspnoea, 8 with persistent abdominal distension and 6 with uncontrolled vomiting who had called multiple times. Not all studies show positive results with teleconsultation for pain. Two systematic reviews showed a benefit of exercise-based telemedicine over no intervention while no significant benefit over usual care, mainly due to lack of evidence.[15,18] In another meta-analysis, there was only moderate-quality evidence that teleconsultation interventions in current times by themselves were not more effective than basic interventions for pain and disability reduction in chronic low back pain.[19]
Fifty-nine out of 547 patients called regarding restocking of the pain medications. Due to restrictions in opioid electronic prescription, they were advised to visit our OPD or visit a local palliative care centre. Communications with other centres were made by our team to guide such patients. There were calls seeking guidance regarding diet, medications, home care, etc. (56), guidance regarding other department appointments (52) and palliative outpatient visit (31).
The major hindrances cited by our patients were inconveniences due to travel ban (49%) including extreme high fares and prohibition to cross state lines, fear of contracting COVID-19 infection (37%) and physical or cognitive constraints (7%). In India, during the lockdown period, the travel-related costs had increased substantially.[13] Because most patients belong to lower financial strata; this was a major hindrance for treatment continuation and an incentive to strengthen telemedicine. Other studies have also pointed out the benefits of telemedicine which include less travel for patients, less disturbance to family members and more economical.[7]
Our institute has an evolving end-of-life care policy in place for registered patients. Three terminally ill patients were provided with terminal care through video conferencing with the attendants. Two patients had shortness of breath, and the third patient had death rattles identified through a video call. All three patients passed away comfortably in their sleep after upgrading the opioid dose. A well-planned study for the utility of this service for a larger cancer patient population from different sociocultural and demographic backgrounds is warranted in the future.
In our study, 74% were very satisfied with the service, and among them, 73% would continue to use this medium in the future. A total of 14 (2.65%) patients were unsatisfied and decided not to avail of this method of treatment in the future. There was no significant difference in satisfaction scores between individuals who consulted once versus those who consulted more than once. It should be noted that among patients who consulted more than once, the satisfaction score for the last call was used for the analysis. In a systematic review on satisfaction levels of patients concerning the usage of telemedicine, it was found that most patients found it acceptable.[20]
Opioid dispensing remains an issue in India as well as other countries through teleconsultation. Ministry of Health and Family Welfare of India in its latest telemedicine guidelines prohibits the prescription of Schedule X drugs, which include narcotics.[8] However, there is a large group of cancer patients whose daily life shall be hampered if they do not have access to opioids through prescription. There is an urgent need for the upgradation of these regulations to make sure patients are not denied their basic right to a pain-free life.[21]
One of the major limitations of this single-centre study was the retrospective nature of the study and the small sample size. Although we provided teleconsultation contact details of various departments to the patients who needed consultation from other concerned facilities, we could not follow up with them to assess whether their queries were answered or not. A real-time multidisciplinary teleconsultation service is the answer to this problem, which was lacking in our setup. To assess the satisfaction level regarding the utility of telemedicine, various aspects such as quality of voice/video, language, advice clarity, politeness and how helpful or cessation of complaints should be delved into. Further studies should be carried out to assess the impact of teleconsultation with follow-up interviews. Further surveys are also warranted to assess the cost analysis of telemedicine for hospitals and patients.
CONCLUSION
Considering the increased susceptibility to severe COVID-19 in patients with cancer, telemedicine can be used as an effective alternative for in-patient follow-ups. There is a need for similar platforms at a secondary and primary level as well to decrease the burden on tertiary care referral hospitals.
Acknowledgements
None.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sector.
Declaration of patient consent
Patient’s consent not required as only medical records were accessed in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Humanitarian telemedicine: Potential telemedicine applications to assist developing countries in primary and secondary care. ESPI Report. 2014;64:39.
- [Google Scholar]
- Providing access to oncology care for rural patients via telemedicine. J Oncol Pract. 2006;2:228-30.
- [CrossRef] [Google Scholar]
- The Evolution of Telehealth: Where Have We Been and Where Are We Going? 2012. The Role of Telehealth in an Evolving Health Care Environment: Workshop Summary. National Academies Press (US); Available from: https://www.ncbi.nlm.nih.gov/books/NBK207141/ [Last accessed on 2020 Jul 21]
- [Google Scholar]
- Virtually perfect? Telemedicine for COVID-19. N Engl J Med. 2020;382:1679-81.
- [CrossRef] [Google Scholar]
- Accelerating telemedicine for cerebral palsy during the COVID-19 pandemic and beyond. Front Neurol. 2020;11:746. Available from: https://www.frontiersin.org/articles/10.3389/fneur.2020.00746/full [Last accessed on 2020 Jul 21]
- [Google Scholar]
- The role of telemedicine during the COVID-19 epidemic in China-experience from Shandong province. Crit Care. 2020;24:178.
- [CrossRef] [Google Scholar]
- Medical oncology clinics through videoconferencing: An acceptable telehealth model for rural patients and health workers. Intern Med J. 2012;42:780-5.
- [CrossRef] [Google Scholar]
- Telemedicine Practice Guidelines. 2020. Enabling Registered Medical Practitioners to Provide Healthcare Using Telemedicine. Available from: https://www.mohfw.gov.in/pdf/Telemedicine.pdf [Last accessed on 2020 Jun 15]
- [Google Scholar]
- Effect of nation-wide lockdown on palliative care services in a tertiary care center in India: A retrospective observational study. Indian J Palliat Care. 2020;26:S45-7.
- [Google Scholar]
- Smartphone-based telemedicine service at palliative care unit during nationwide lockdown: Our Initial experience at a tertiary care cancer hospital. Indian J Palliat Care. 2020;26:S31-5.
- [Google Scholar]
- Countries with Most WhatsApp Users 2019. Statista. Available from: https://www.statista.com/statistics/289778/countries-with-the-most-facebook-users/ [Last accessed on 2020 Jul 21]
- [Google Scholar]
- 'A Friend in the Corner': Supporting people at home in the last year of life via telephone and video consultation-An evaluation. BMJ Support Palliat Care. 2019;9:e26.
- [Google Scholar]
- Patients'/caregivers' perspectives on telemedicine service for advanced cancer patients during the COVID-19 pandemic: An exploratory survey. Indian J Palliat Care. 2020;26:S40-4.
- [Google Scholar]
- Internet interventions for chronic pain including headache: A systematic review. Internet Interv. 2016;4:17-34.
- [CrossRef] [Google Scholar]
- Tailored web-based interventions for pain: Systematic review and meta-analysis. J Med Internet Res. 2017;19:e385.
- [Google Scholar]
- Telemedicine in the Era of COVID-19. J Allergy Clin Immunol Pract. 2020;8:1489-91.
- [CrossRef] [Google Scholar]
- Interactive telemedicine: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2015;2015:CD002098.
- [Google Scholar]
- The effectiveness of exercise-based telemedicine on pain, physical activity and quality of life in the treatment of chronic pain: A systematic review. J Telemed Telecare. 2018;24:511-26.
- [CrossRef] [Google Scholar]
- Effectiveness of telehealth-based interventions in the management of non-specific low back pain: A systematic review with meta-analysis. Spine J. 2017;17:1342-51.
- [CrossRef] [Google Scholar]
- Systematic review of studies of patient satisfaction with telemedicine. BMJ. 2000;320:1517-20.
- [CrossRef] [Google Scholar]
- Opioid prescribing in the midst of crisis-Myths and realities. N Engl J Med. 2020;382:1086-8.
- [CrossRef] [Google Scholar]




