
Translate this page into:
Recommendations to Support Nurses and Improve the Delivery of Oncology and Palliative Care in India
Address for correspondence: Dr. Virginia T LeBaron, Department of Acute and Specialty Care, University of Virginia School of Nursing, 202 Jeannette Lancaster Way, McLeod Hall Charlottesville, VA 22903, USA. E-mail: vlebaron@virginia.edu
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Nurses in India often practice in resource-constrained settings and care for cancer patients with high symptom burden yet receive little oncology or palliative care training.
Aim:
The aim of this study is to explore challenges encountered by nurses in India and offer recommendations to improve the delivery of oncology and palliative care.
Methods:
Qualitative ethnography.
Setting:
The study was conducted at a government cancer hospital in urban South India.
Sample:
Thirty-seven oncology/palliative care nurses and 22 others (physicians, social workers, pharmacists, patients/family members) who interact closely with nurses were included in the study.
Data Collection:
Data were collected over 9 months (September 2011– June 2012). Key data sources included over 400 hours of participant observation and 54 audio-recorded semi-structured interviews.
Analysis:
Systematic qualitative analysis of field notes and interview transcripts identified key themes and patterns.
Results:
Key concerns of nurses included safety related to chemotherapy administration, workload and clerical responsibilities, patients who died on the wards, monitoring family attendants, and lack of supplies. Many participants verbalized distress that they received no formal oncology training.
Conclusions:
Recommendations to support nurses in India include: prioritize safety, optimize role of the nurse and explore innovative models of care delivery, empower staff nurses, strengthen nurse leadership, offer relevant educational programs, enhance teamwork, improve cancer pain management, and engage in research and quality improvement projects. Strong institutional commitment and leadership are required to implement interventions to support nurses. Successful interventions must account for existing cultural and professional norms and first address safety needs of nurses. Positive aspects from existing models of care delivery can be adapted and integrated into general nursing practice.
Keywords
Chemotherapy
India
nurses
oncology
palliative care
recommendations

INTRODUCTION
The global cancer burden is rapidly increasing and is projected to dramatically affect low- and middle-income countries (LMICs) in the coming decades.[1234] It is estimated that by 2030, the number of cancer deaths worldwide will increase by almost 80%, with the majority occurring in LMICs.[5] In India, approximately 1 million people are diagnosed with cancer each year and close to 700,000 died from the disease in 2012.[6] Almost 70% of patients in LMICs, including India, are diagnosed with late-stage cancer and require excellent palliative care to manage multiple symptoms.[5]
The growing burden of cancer in the developing world is poised to strain the already heavy workload of nurses in LMICs and exacerbate serious healthcare workforce shortages.[78910] Worldwide, nurses comprise the largest group of healthcare providers.[11] It is essential that feasible, sustainable, and specific strategies to support nursing practice in LMICs are implemented to improve patient care outcomes, address the exploding rates of noncommunicable diseases, and meet the United Nations health-related sustainable development goals.[1112131415] However, this is not an easy task as nurses who provide cancer care in LMICs face numerous challenges, including an overwhelming volume of highly symptomatic patients, limited access to essential supplies and medications, lack of specialized oncology and palliative care training, and institutional and professional dynamics of power, stigma, and hierarchy that can make the nurse feel disempowered and helpless.[910161718192021]
The broader sociocultural and political challenges that affect health care delivery in government hospitals in India are complex and do not have simple solutions. Continuing to improve governmental policy (at both the state and national level) should be an ongoing goal to help nurses and patients. However, one must balance this goal with the reality that this level of change can take significant time. Consequently, the goal of this report is more modest: to propose hospital-level recommendations to support nurses who practice in India, with the hope that this will, in turn, improve outcomes for cancer patients in LMICs. The following recommendations are intended to capitalize on existing strengths and be constructive, pragmatic and implemented at the institution/hospital level.
METHODS
This report describes recommendations for nursing practice that were identified as a part of a larger ethnographic study that explored nurse moral distress and cancer pain management in India.[1622] The challenges and opportunities discussed below are based on interviews and observations collected during 9 months of in-country immersion fieldwork by the first author.
Design
Methods for the parent study have been described in detail elsewhere.[1622] In brief, the original project was a qualitative, ethnographic study designed to explore the experiences of nurses who care for patients with advanced cancer in India.
Setting
South Indian Cancer Hospital (SICH [A pseudonym is used to protect the identity of the institution and research participants]) is a 300-bed government/public sector cancer hospital in urban South India known to the first author through previous collaborations. Typical of government sector hospitals in India, SICH serves a predominantly impoverished population and faces serious resource shortages. SICH is the only government cancer hospital in the state, and many patients travel from far distances to receive treatment. The hospital accepts approximately 10,000 new patients a year, and the majority of patients present in the late stages of cancer, with a high symptom burden. Inpatients are admitted to the general wards (surgical or medical), pediatrics, or Intensive Care Unit (ICU) and there is a large outpatient clinic population (radiation, medical oncology, surgical oncology, palliative care). At the time this research was conducted there were 79 bedside nurses (including head nurses, government nurses, and contract nurses) and 1 nursing superintendent employed at SICH. Currently, there are 10 head nurses, 64 government staff nurses, 36 contract staff nurses, and 1 nursing superintendent.
Data collection
Participants were recruited using an informational flyer (written in the local language) distributed at a meeting with the nursing staff, through interactions during observational experiences, and by word of mouth. Data were collected over 9 months from September 2011 through June 2012. Consistent with the principles of ethnography, data collected consisted primarily of observations and interviews.[232425] A key goal was to collect data from different sources that could be used for corroboration and comparison.[2627]
Interviews were approximately 1 hour in length and audio-recorded with permission. A translator assisted as needed. Interview questions were open-ended and designed to allow the participant to talk freely about their experiences caring for cancer patients. During interviews and informal conversations, the first author asked participants questions such as, “What could help make your job better or easier?” Many participants had a difficult time answering this question, but some nurses had very specific suggestions as to how to improve patient care and were eager to share their thoughts.
Observations involved “shadowing” (closely following) nurses in their day-to-day care of patients. Most (but not all) of the nurses shadowed were also formally interviewed. Observations were recorded in the field as small notes (or memos) and then expanded into larger, written explanations of the observations each evening (known as “field notes”).[24]
Data analysis
Formal interviews were transcribed and accuracy of translation was verified by two independent speakers of the local language. The translated interviews were analyzed using a qualitative software program (Dedoose version 4.5.91) to organize the text to answer specific questions and identify the main messages or themes.[16] Field notes were organized chronologically and iteratively analyzed for patterns that confirmed or contradicted interview findings. Field note and interview data were integrated into a narrative account that addressed the a priori research questions. The results from data analysis were validated with participants informally during fieldwork and formally at the completion of fieldwork through a hospital-wide presentation.
Ethical considerations
Institutional Review Board (IRB) approval was obtained from both the University of Utah (USA) and the SICH Ethics Committee before data collection. The project was also reviewed and approved by the Government of India. Participants who agreed to be formally interviewed were verbally consented using an IRB approved consent form in both English and the local language. No financial compensation was offered, but participants who were formally interviewed received a small gift of appreciation (valued at approximately Rs. 700, $10 USD). Participant identity was disguised, and location and identifying details were altered to protect confidentiality.
RESULTS AND DISCUSSION
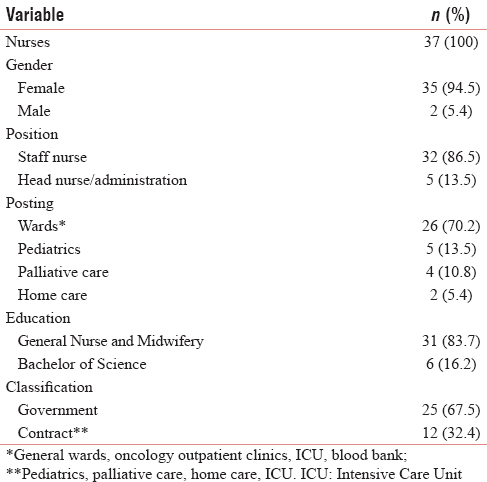
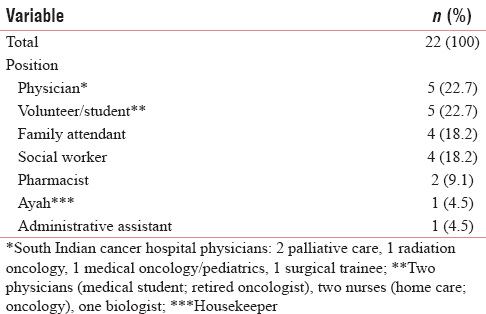
A total of 54 (n = 54) formal, semi-structured interviews were conducted. Of these 54 interviews, 37 (n = 37) nurses from SICH were formally interviewed, as well as 22 (n = 22) other caregivers (physicians, pharmacists, etc.) who work closely with nurses [Tables 1 and 2]; some participants were interviewed more than once. In addition, over 400 hours of observations were conducted, mostly at SICH. Limited observations for comparison were also conducted at two other local government hospitals (a nearby maternal and child health hospital and a general hospital), one private/corporate cancer hospital, one trust cancer hospital, and also with rural outreach, hospice, and home care teams.
The primary study findings that address the research questions related to nurse moral distress and access to pain relief have been reported elsewhere[1622] and are not the focus of this report. Instead, this report focuses on sources of work-related distress experienced by the nurses in a government cancer hospital in India and institution-level recommendations to help support nurses in their care of cancer patients. The key recommendations identified to support nurses in India include: prioritize safety, optimize the role of the nurse and explore innovative models of care delivery, empower staff nurses, strengthen nursing leadership, offer relevant educational programs, enhance teamwork, improve cancer pain management, and engage in research and quality improvement projects.
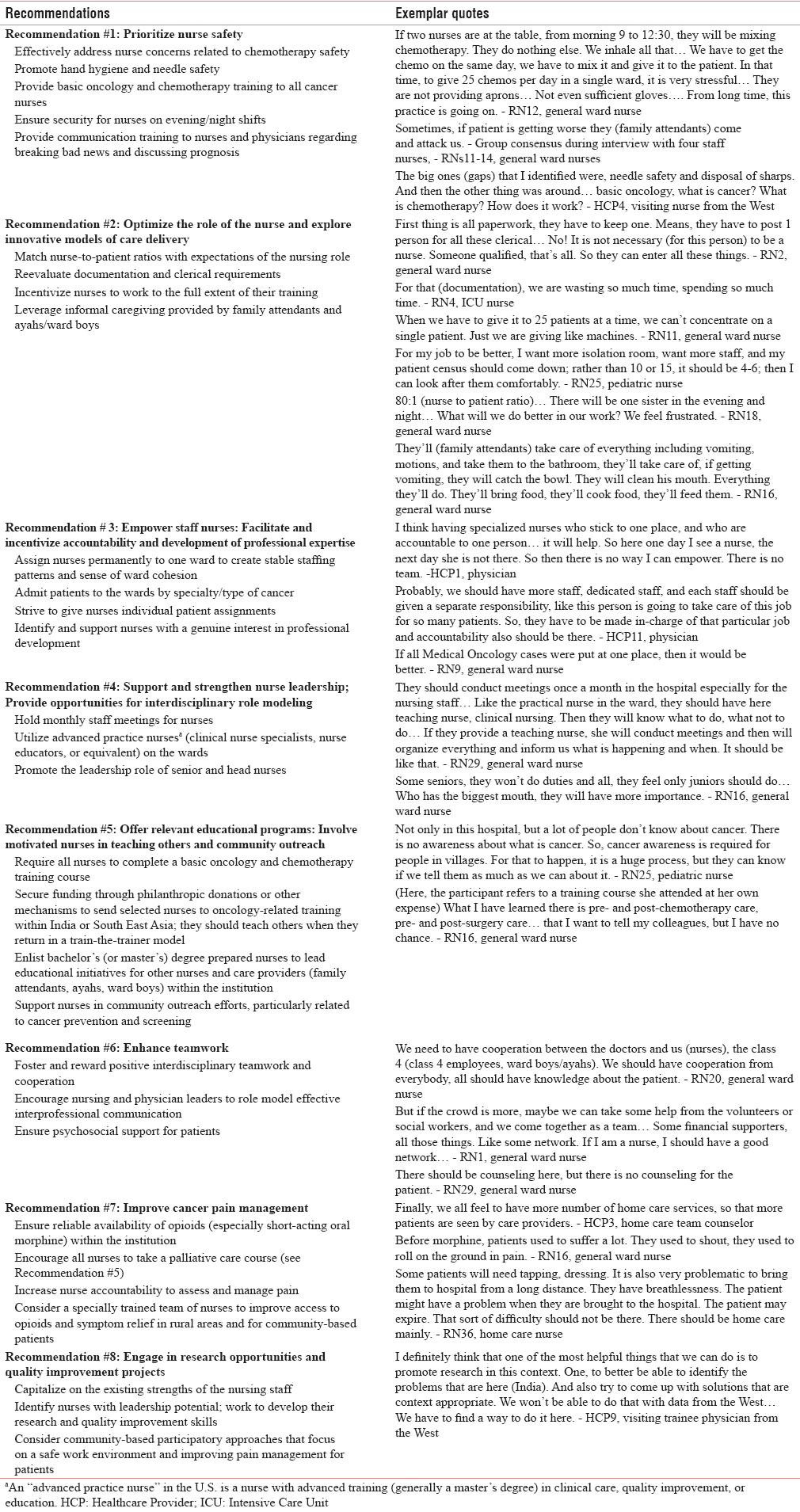
Each recommendation is described below by detailing the specific challenge and opportunities. Except recommendation #1, which is felt to be the most urgent priority and is therefore listed first, the additional recommendations are considered equally important and are not ranked in any particular order. Hospital directors may wish to review the list, ideally in consultation with their nursing colleagues, and focus efforts on priorities most relevant for their specific institution. Table 3 provides a summary of the recommendations, along with supporting quotes from participants.
Recommendation #1: Prioritize nurse safety
Challenge
Two primary safety concerns for nurses emerged from the data: (1) occupational hazards related to lack of supplies and chemotherapy administration and (2) perceived risk of personal workplace violence/harassment.
Lack of supplies and chemotherapy administration
Many nurses were distressed by the lack of supplies, such as thermometers, bedpans, and wheelchairs. Lack of basic resources (such as running water or soap) compromised the safety of nurses and patients and made it extremely difficult to implement fundamental elements of nursing practice, such as good hand hygiene, which has been demonstrated to be the most important front-line strategy in reducing the spread of infection in hospitals.[28]
Another critical safety issue, voiced by almost every nurse, involved the mixing and administration of chemotherapy, which occurred without access to a ventilation hood or appropriate personal protective equipment. Most nurses feared for their physical health related to exposure to chemotherapy (and to a lesser extent, radiation) and verbalized some understanding of the risks. Many expressed specific concerns about how exposure could affect their menstrual cycles, fertility, and ability to carry a child. These concerns are legitimate and well documented in current guidelines.[29303132]
Opportunities
Providing appropriate incentives and accountability for nurses to engage in regular, between-patient hand sanitization (such as with hand sanitizer gel if sinks/water are not easily accessible) is important to prevent infection among vulnerable cancer patients whose immune systems are weakened by the effects of chemotherapy, radiation, and surgery. Supplies that directly relate to patient and nurse safety (for example, gloves, soap, “sharps” containers to dispose of used needles) are essential and increased accountability related to their use is recommended. Hospital administrations and senior personnel can work to ensure that these resources are available and utilized by nurses, other healthcare providers, and family attendants (family members). For example, at a pediatric public hospital in Nepal, V.L. observed that the primary family attendant was provided with a bottle of hand sanitizer that was kept at the patient's bedside; the family attendant was tasked with offering hand sanitizer to every care provider that approached the patient.
Safety issues related to chemotherapy are important for all staff who handle and administer chemotherapy, but they are particularly essential for nurses directly involved in the reconstitution and mixing of chemotherapy agents, and who are at high risk for repeated exposure through inhalation, dermal absorption, or ingestion.[30] Some have called for LMIC hospitals to prioritize hiring dedicated pharmacists or pharmacy technicians to assume the task of mixing chemotherapy, thereby removing this activity from the work of nurses.[10] While this could be an important strategy, it is often complicated by a lack of trained pharmacists and available safety equipment[89] and perceived role expectations of the nurse. In the meantime, one idea is to mandate pharmaceutical companies who distribute chemotherapy agents to institutions such as SICH to include adequate amounts of personal protective equipment (gloves, aprons, masks, eye protection) for nurses along with their shipments and require senior and head nurses to ensure they are properly used.
It is important to note that larger system issues related to safe disposal of bio-hazardous waste are a crucial environmental and safety issue that needs to be addressed by the local and state government. However, most urgently, hospital staff, patients, and family attendants must be protected from unnecessary exposure to cytotoxic agents and needle-sticks while in the hospital, and effective strategies can be simple and cost-effective. For example, chemotherapy mixing tables in the wards could be moved further away from patients and family members and closer to windows and fans for improved ventilation; basic wooden ventilation hoods could be constructed to make chemotherapy mixing safer for nurses, and family members discouraged from handling chemotherapy. Nurses could be provided with inexpensive, reusable, plastic point-of-use trays, so they are able to keep sharps more safely contained as they move bed-to-bed, patient-to-patient (this last strategy was piloted on the pediatric wards by Z.L. during a trip to SICH with significant success).
Providing basic chemotherapy safety training for nurses (and any other caregivers involved in handling chemotherapy) could be done cost-effectively by exploring local or regional chemotherapy training programs that already exist, partnering with nongovernmental organizations or other nonprofit training institutions, or through an international “twinning program” with oncology certified and specialist nurses who are informed and sensitive to the realities of practice in LMICs.[33] Particular attention should be given to chemotherapy dose calculations and prevention of chemotherapy extravasations and needle-sticks. Education about safe needle practices and tools to help nurses administer medications and insert intravenous lines with less risk of getting accidently punctured (”stuck”) by used needles is needed. Nurses (as well as auxiliary staff and family attendants who are likely to be monitoring chemotherapy infusions on an overcrowded ward) must be taught to promptly recognize the signs and symptoms of extravasation and how to properly intervene to prevent potentially devastating complications.
Perceived risk of personal workplace violence
Nurses expressed fear that family attendants would verbally or physically attack them if a patient's clinical status deteriorated or a patient died unexpectedly during their shift. Female nurses seemed especially concerned about their personal safety during evening or night shift when staffing and security were minimal. Other female nurse participants did not express explicit concerns for their personal safety, but a more general discomfort in attending to the personal care needs of male patients.
Opportunities
Nurses’ fear of personal violence in the hospital is not unique to India and has deep and complex roots, including disconnection between nurses and family attendants, lack of information or misunderstandings by family attendants regarding patient prognosis, frustrations related to overcrowding and understaffing, and societal perceptions and stereotypes regarding gender, status/class, and the profession of nursing.[161734] Strategies to address this concern are equally complex, but a first step could include acknowledging the nurses’ fears in a formal meeting with hospital leadership and increasing meaningful security presence at night within hospital wards. Promoting opportunities for positive interactions between nurses and family attendants, as well as training physicians and nurses to effectively discuss prognosis and break bad news to family members, represent longer term and upstream strategies to help address concerns of personal violence. Hiring a diverse nursing workforce, to include more male nurses, is also a potential strategy.
Recommendation #2: Optimize the role of the nurse and explore innovative models of care delivery
Challenge
Almost all nurses discussed stress related to nurse-to-patient staffing ratios. Many felt that increasing the number of nurses was a crucial factor to improve patient care, particularly on evening and night shifts. Ratios on the general wards of one nurse to sometimes over fifty patients are extremely challenging/impossible, and by default, reduce the nurse to a medication technician and clerical scribe. “No time” was the primary reason given by nurses to explain compromised patient care. Most nurses expressed that they found the amount of required documentation tedious and the major barrier to having time to provide direct care to patients.
Opportunities
Increasing the number of nurses is recommended in combination with reexamining the roles and responsibilities of the nurse. In other words, hiring more nurses to allow for better nurse-to-patient ratios is an important step, but it is not enough by itself. Hiring additional nurses will be more successful if it is accompanied by concurrent efforts to encourage and incentivize nurses to practice to the full extent of their training and capacity. Supporting nurses to realize their full scope of practice will require commitment by hospital leadership and buy-in from senior nursing staff.
One way to give nurses in the current system more time to care for patients is to reexamine the type and amount of documentation required and who is responsible for it. Much of the currently required documentation is redundant and has a debatable role in improving patient care. One senior nurse suggested that the burden of clerical work could be largely delegated to nonnursing personnel. Reducing clerical work may alter the “identity” of general ward nurses, and a period of intensive role modeling may be necessary to help nurses focus on patient-centered aspects of their job that can occupy time previously dedicated to documentation.
It is unlikely that the large patient-to-nurse ratios in LMIC public sector hospitals will improve in the near future; in fact, they will likely worsen as the global burden of cancer and other noncommunicable diseases explodes. Therefore, it is critical that pragmatic, scalable, and novel care delivery models are implemented and evaluated. For example SICH in a family attendant is required to remain in the hospital for the patient to receive care. Family attendants, along with ayahs (housekeepers) and ward boys (orderlies), informally perform and assist with many crucial nursing-oriented tasks, such as medical administration, dressing changes, toileting, and mobilizing patients. New models of care delivery that formally train, support, and leverage the activities of the family attendant and auxiliary staff[353637] can provide cost-effective approaches to improve patient care in hospitals such as SICH; more resources and funding should be directed towards implementing and evaluating such models.
Recommendation #3: Empower staff nurses: Facilitate and incentivize accountability and development of professional expertise
Challenge
Nurses in this study, particularly those on the general wards (versus specialty departments, such as pediatrics or palliative care), reported limited opportunities and incentives to develop their professional expertise.
Opportunities
Many nurses expressed eagerness to enhance their professional skillset; such individuals could be organized into an informal “professional development team” to help improve care delivered at the bedside. Examples of specific strategies to enhance accountability, continuity of care, and foster the development of professional nursing identity include: assigning nurses permanently to a specific ward to create stable staffing patterns (versus requiring nurses to shift/rotate wards every few months); assigning/admitting patients to the wards by specialty/type of cancer to help nurses develop proficiency and expertise in caring for a specific cancer population, such as medical oncology patients; and give nurses individual patient assignments, when possible, to increase nurse accountability and the connection between the nurse and patient/family attendant.
Nurses who demonstrate an eagerness to enhance their skill set and leadership potential should be identified by hospital administrators, given more decision-making authority, and provided with opportunities and financial support for professional development, expecting that they will formally share this knowledge with colleagues.
Recommendation #4: Support and strengthen nurse leadership; Provide opportunities for interdisciplinary role modeling
Challenge
Participants expressed concerns regarding strained interactions between different groups of interdisciplinary care providers, limited decision-making opportunities for nurses, and an emphasis of seniority over competence.
Opportunities
Certain departments within SICH have the benefit of particularly strong physician leadership and advocacy; this results in greater support and additional professional development opportunities offered to nurses working in these departments. Importantly, these physicians provide excellent role modeling for nurses related to communication with patients and family attendants and a commitment toward solving difficult patient care problems. Identified physician champions for nurses should be formally recognized and supported by hospital leadership.
There is great potential for senior and head nurses to assume increased responsibilities in the development of junior staff through role modeling and promotion of professional standards. Similar to staff nurses who could be permanently assigned to one ward, head nurses could also be permanently assigned to one ward (versus shifting/rotating from ward to ward). This may foster an increased sense of accountability and continuity in the supervisory management and professional development of junior nursing staff.
One participant (who had significant nursing experience in the private sector and also abroad) suggested that regular staff meetings and educational activities for nurses are important and should be organized for nurses at SICH; this is a role that head nurses could potentially assume, with appropriate mentorship. This participant also suggested that a “teaching nurse” should be available on the wards to support nurses. This suggestion seems consistent with the employment of a clinical nurse specialist (CNS) or nurse educator (terms used in the United States or Canada) – a nurse with advanced training who can help teach and guide other nurses in best practices and quality improvement efforts.[38] One strategy for government hospitals in India could be to prioritize employment of two Master's prepared nurses (either from within India or from another country or similar setting) to help supervise clinical practice, write protocols and standards of care, and role model patient-centered care. Clearly, this represents a financial investment for the hospital, but there are cost-effective and creative ways to explore this possibility. For example, it may be possible to partner with a College or School of Nursing, either from within India or internationally, who offers academic credit to graduate nurses for this type of practicum global health work. Additional “twinning” partnerships could be sought within professional organizations that have a commitment to global oncology nursing, such as the International Society for Nurses in Cancer Care.[39] Long-term immersion in the field by a nursing mentor, or team of nursing mentors, sensitive to the on-the-ground realities and cultural context of the specific LMIC setting, could be a helpful strategy to role model caring and advocacy behaviors.[4041]
Recommendation #5: Offer relevant educational programs: Involve motivated nurses in teaching others and community outreach
Challenge
Nurses are on the frontlines of managing cancer treatment and symptoms, but most of them do not receive formal training related to oncology care.
Opportunities
There are many educational topics relevant for cancer nurses in India, especially related to palliative care and chemotherapy. Standardized, general content regarding cancer biology, treatment modalities, symptom management, and palliative care should be integrated into preclinical level (e.g., General Nurse and Midwifery (GNM), and BSc) nursing curricula.[42] A more specialized, standardized chemotherapy certification course (that focuses on safe chemotherapy mixing and administration, managing treatment side effects, and oncologic emergencies) should be required for all government and private sector oncology nurses who administer chemotherapy. Curricula models exist that cover general oncology topics, as well as specific palliative care and chemotherapy content;[43444546] however, most are based on high-income country resources. It is critical that any oncology nurse curriculum or chemotherapy certification course developed for India (or any LMIC) is culturally and contextually relevant, developed and ultimately taught by in-country leaders to ensure sustainability, and involves hands-on, mentored practice at the bedside.[10162147]
One excellent example of a relevant in-country training course is the month long palliative care course offered at SICH, which has been completed by all of the palliative care department nurses and a limited number of the general ward nurses. A modified and abbreviated version of this course, which emphasizes pain assessment and management, care of the actively dying patient, and communication, is recommended for all cancer nurses in India. General ward nurses should be taught basic principles regarding the safe and beneficial use of morphine even if they are not administering the medication themselves. Obviously, this requirement could strain existing resources (in terms of time needed to teach the class and nurses being away from their wards), and support would need to be granted at the institutional level. Exploring telehealth and e-learning delivery models may be an option depending on the institution's technology and internet capabilities. However, meeting this goal could also promote nursing development as the classes could be taught by nurses who have already completed the training and who can role model to others effective ways to communicate and manage symptoms. A train-the-trainer approach that capitalizes on local expertise and cultural knowledge is essential. Such an approach has the potential to empower nurses and improve patient care by focusing on the types of scenarios nurses typically encounter at hospitals such as SICH. For example, most Western nurses (except specially trained wound and ostomy nurses) have limited knowledge about how to manage the complicated wounds often seen in LMICs; SICH palliative care nurses are already experts in this area and have much knowledge to share with nursing colleagues. Another potential benefit of a train-the-trainer model is that it may foster greater cooperation and collegiality between distinct groups of nurses within an institution (for example, between contract nurses and government appointed nurses). At SICH, many lay-providers, such as volunteers and family attendants, and ayahs and ward boys care for patients; these individuals could also be involved in nurse-led educational programs to learn about symptom management and caring for cancer patients; such a program may be a positive step to further improve interactions between family attendants, ayahs/ward boys, and nurses.
A number of nurse participants also discussed their interest in educating members of the community about cancer screening and prevention. This is an area ripe for nurse leadership as it is a project well aligned with the professional goals of nursing and has the potential to make a significant and positive impact on the local community. Nurses who have an interest in this type of community outreach should be identified, and a nursing leader, ideally within the home institution, could be assigned to coordinate and facilitate this professional activity.
Recommendation #6: Enhance teamwork
Challenge
Many nurses talked about the importance of “teamwork” and believed that more could be accomplished by working together. However, a strong sense of hierarchy and segregation among physicians, nurses, class IV employees (ward boys and ayahs), and patients and family attendants within the hospital (observed during fieldwork) may create barriers to cooperation as equal team members. Nurses, especially on the general wards, expressed distress related to professional isolation and lack of supportive services. The absence of counseling services to help patients and family attendants cope with the tremendous psychosocial and financial impact of cancer was mentioned by a number of nurses (and other healthcare providers), who felt like this was an important element of the “team” missing on the general wards.
Opportunities
While it would be naïve to ignore the reality of longstanding power dynamics, certain measures can be taken to enhance a sense of teamwork. For example, working together to offer interdisciplinary education (see Recommendation #5) may be one way. Nursing leaders could role model collegial, interdisciplinary collaboration between different groups of nurses within the hospital and with physicians and ward boys and ayahs. Physician champions within a hospital can engage nurses collaboratively on patient rounds and role model effective interdisciplinary and patient-provider communication.
It may be an extremely beneficial investment for hospitals to enhance social work and counselor support to improve patient care and reduce the risk of nurse burn-out.
Recommendation #7: Improve cancer pain management
Challenge
Opioids, such as morphine, are critical to manage cancer pain, but access to these medications is often problematic in LMICs.[4849505152] Progress has been made to improve opioid availability within India, but many patients with cancer still suffer in avoidable pain.[535455] For example, the palliative care department at SICH has made significant effort to procure morphine and make the medication available to patients, especially those seen in the palliative care department. However, most nurses on the general wards reported (and were observed to have) a very limited role in pain assessment and management and rely on family attendants and the palliative care department to assess and manage pain.[22] This unfortunately results in many patients suffering in pain even when morphine is available in the hospital. Many patients and family members live in rural areas and must travel hundreds of kilometers to reach hospitals such as SICH and obtain morphine.
Opportunities
The first critical step is for hospitals to take action to procure morphine and to ensure, at a minimum, that oral, immediate-release (short-acting) morphine is available at all times in the hospital pharmacy. Institutions that have been successful in procuring morphine (such as SICH) could serve as role models and mentors to other institutions who wish to improve access to pain relief for their patients. Resources exist through international organizations, such as the Pain and Policy Studies Group,[56] as well as regional institutions, such as the Indian Association of Palliative Care[57] and Pallium India,[58] to support improving access to opioids.
Concurrent with ensuring availability of morphine, institutions could require all oncology nurses to complete a basic palliative care course (See Recommendation #5) to improve their ability to appropriately and safely assess and manage pain. Another approach may be to train a motivated group of ward nurses and formally designate and recognize these individuals as “palliative care champions” or “pain resource nurses.” These nurses could then serve as resources and mentors to other nurses on the wards. Similar approaches have been used in higher-resource settings[59] and may be useful in hospitals in India, with appropriate adaptations to account for available resources and cultural differences.
In addition, clinical practice should facilitate nurse accountability for assessing and managing pain. On the general wards, this would likely involve education of the nurses and also a reevaluation of staffing patterns and nursing role expectations (see Recommendation #2). A serious commitment on the part of hospital leadership will be essential for success. On wards where nurse-to-patient ratios are more manageable (such as ICUs, for example), implementing this recommendation could involve education about considering pain as “the 5th vital sign,”[60] improving accurate documentation of patient's pain, and reinforcing the importance of reassessing the effectiveness of pain medication therapy. This type of quality improvement project could be undertaken by a graduate nursing student or nurse educator/CNS (see Recommendation #4).
More than 70% of the Indian population lives in villages,[61] and these individuals are at particular risk of dying in pain. Serious consideration should be given to creating specially trained teams of hospital-based nurses to improve distribution of morphine among rural patients in India as has been done in countries like Uganda.[62] A project such as this is obviously a large undertaking on multiple levels. Government officials and hospital directors could look to successful African models and pilot a program in regions with an existing palliative care network, and a strong history of advocacy and policy work related to opioid availability, such as Kerala or Telangana/Andhra Pradesh.[636465]
Recommendation #8: Engage in research opportunities and quality improvement projects
Challenge
More research is needed to move beyond “transplanting” or “adapting” Western-developed interventions to LMICs and to instead develop a robust evidence base from within LMICs that is culturally, contextually, historically, and linguistically relevant to nurses practicing in these settings.
Opportunities
Future projects should consider a community-based participatory research approach, which actively engages nurses to set priorities and collaboratively develop and pilot solutions. Successful examples of this approach exist in LMICs.[186667] Nurse researchers from higher resource countries involved in twinning programs or related partnerships can work collaboratively and longitudinally with cancer nurses in India to identify priorities and implement realistic interventions and solutions and strive for full ownership of the project to ultimately rest with local in-country collaborators.[68]
Limitations
This study took place in a government/public cancer hospital in India and thus may be most relevant to similar care settings. However, while the available resources and patient population served differ significantly between government/public sector and private/corporate hospitals, many of the concerns voiced by nurses in this report can apply broadly to LMICs and are not unique to government sector hospitals or to India. For example, concerns regarding chemotherapy safety and limited oncology training are likely to be pertinent for many LMIC nurses, regardless of specific practice setting or location.
CONCLUSIONS
Our findings contribute to the body of literature regarding the critical role of cancer nurses in LMICs.[891069] We offer specific institution-level recommendations supported by ethnographic data and designed to improve oncology nursing practice and the care of cancer patients in India.
Efforts to address safety and supply issues by institutional leadership would visibly demonstrate that the role and safety of the nurse are valued and respected. We argue, as have others, that it is unfair to expect nurses to value the safety of patients when their own safety is compromised.[19] Consistent exposure to safety challenges such as those described above, and the feeling that nothing appears to be improving, can contribute to decreased staff morale, poor motivation, and passivity on the part of nursing staff.[70] Hospital leaders could do much to improve nurse morale by taking visible and relatively simple, but meaningful steps to provide a safer working environment for nurses.
Specifically, safety needs for nurses, family attendants, patients, and auxiliary staff (ayahs and ward boys) related to chemotherapy mixing and administration should be a top priority; cost-effective and pragmatic strategies exist to address this challenge. Standardized basic training in cancer biology, cancer treatment and side effect management, and safe handling of cytotoxic agents should be required of all nurses administering chemotherapy, regardless of setting or location. Additional steps include supporting the professional development and scope of practice of oncology nurses through appropriate mentorship, recognition, and role modeling; aligning nurse leadership and decision-making authority to a greater degree with competency versus seniority; and developing workforce capacity strengthening interventions from within the LMIC setting using a community-based participatory approach to ensure cultural relevance and sustainability.
It is also critical to acknowledge the positive work that already occurs at SICH (and other hospitals in India) and the commitment to progress by the hospital leadership and administration. The majority of cancer patients who present for care in India have serious and significant needs – physically, emotionally, and socially, and it is extremely difficult work. The hospital leadership and all healthcare providers fulfill a crucial role in helping these patients and family members. It is hoped that this report can build upon the existing strengths and positive work at SICH and other hospitals in India by offering constructive and helpful recommendations to further improve patient care and support to nurses.
Supporting nurses who practice in LMICs is crucial since they will increasingly care for a growing number of patients with cancer. It is vital for hospital administrators and government officials to first address the difficult working conditions and safety needs of oncology nurses in India and similar settings so that there is an opportunity to actualize the full potential of nursing practice.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We thank Dr. Kristin Cloyes, Dr. Patricia Berry, Dr. Martha Maurer, Dr. Fraser Black, Dr. Mark Nitcher, and The International Network for Cancer Treatment and Research for their support and encouragement of the project. We are especially grateful to all of the staff and nurses of South Indian Cancer Hospital who shared their experiences that helped form the basis of this report.
REFERENCES
- 2016. World Health Organization (WHO). Global Health Observatory Data, Noncommunicable Diseases. Available from: http://www.who.int/gho/ncd/en/
- American Cancer Society. Global cancer facts and figures (3rd ed). Atlanta: American Cancer Society; 2015.
- Expansion of cancer care and control in countries of low and middle income: A call to action. Lancet. 2010;376:1186-93.
- [Google Scholar]
- Inside India's Cancer Epidemic. 2014. Cancer World. Available from: http://www.cancerworld.org/pdf/4909_pagina_22_28_Best_Reporter.pdf
- [Google Scholar]
- 2014. Centers for Disease Control and Prevention (CDC). Global Cancer Burden. Available from: http://www.cdc.gov/cancer/international/burden.htm
- The growing burden of cancer in India: Epidemiology and social context. Lancet Oncol. 2014;15:e205-12.
- [Google Scholar]
- 2013. A universal truth: No health without a workforce. Geneva: World Health Organization; Available from: http://www.who.int/workforcealliance/knowledge/resources/GHWA-a_universal_truth_report.pdf?ua=1
- Nursing's potential to address the growing cancer burden in low- and middle-income countries. J Glob Oncol. 2016;2:154-63.
- [Google Scholar]
- Key Stakeholder Group on Oncology Nursing in Low- and Middle-Income Countries. Strengthening the oncology nurse workforce in low-income and middle-income countries. Lancet Oncol. 2015;16:887-8.
- [Google Scholar]
- 2013. Enhancing nursing and midwifery capacity to contribute to the prevention, treatment and management of noncommunicable diseases. Human Resources for Health Observer. Geneva: World Health Organization; Available from: http://www.who.int/hrh/resources/observer 12/en/
- 2013. World Health Organization (WHO) Nursing and Midwifery Progress Report 2008-2012. Available from: http://www.who.int/hrh/nursing_midwifery/progress_report/en/
- Promoting cancer nursing education, training, and research in countries in transition. In: Silbermann M, ed. Cancer Care in Countries and Societies in Transition. Switzerland: Springer International Publishing; 2016. p. :473-93.
- [Google Scholar]
- 2016. International Council of Nurses Calls for Investment in Nursing and Midwifery. Available from: http://www.intlnursemigration.org/2016/06/international-council-of-nurses-calls-for-investment-in-nursing-and-midwifery/
- Global advisory panel on the future of nursing (GAPFON) and global health. J Nurs Scholarsh. 2015;47:3-4.
- [Google Scholar]
- Nurse moral distress and cancer pain management: An ethnography of oncology nurses in India. Cancer Nurs. 2014;37:331-44.
- [Google Scholar]
- 2006. A Profession on the Margins: Status Issues in Indian Nursing: Centre for Women's Development Studies. Available from: https://archive.nyu.edu/handle/2451/34246
- Moral distress among Ugandan nurses providing HIV care: A critical ethnography. Int J Nurs Stud. 2010;47:723-31.
- [Google Scholar]
- Improvising Medicine: An African Oncology Ward in an Emerging Cancer Epidemic. Duke University Press; 2012.
- Enhancement of oncology nursing education in low-and middle-income countries: Challenges and strategies. J Cancer Policy. 2016;8:10-6.
- [Google Scholar]
- An ethnographic study of barriers to cancer pain management and opioid availability in India. Oncologist. 2014;19:515-22.
- [Google Scholar]
- Critical Ethnography: Method, Ethics, and Performance. Thousand Oaks, CA: SAGE Publications; 2005.
- Writing Ethnographic Fieldnotes. University of Chicago Press; 1995.
- Ethnography: The method. Nursing Research: A Qualitative Perspective. Jones and Barlett Publishers; 2012. p. :285-335.
- The World Health Organization Guidelines on Hand Hygiene in Health Care and Their Consensus Recommendations. 2009. World Health Organization. :611-22. Available from: http://www.whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf
- [Google Scholar]
- 2012. Centers for Disease Control and Prevention (CDC), National Institute for Occupational Safety and Health (NIOSH). Occupational Exposure to Antineoplastic Agents. Available from: http://www.cdc.gov/niosh/topics/antineoplastic/
- 2013. World Health Organization (WHO) and Pan American Health Organization (PAHO). Safe Handling of Hazardous Chemotherapy Drugs in Limited-Resource Settings. Available from: http://www.paho.org/hq/indexphpoption=com_docman&task=doc_view& Itemid=270&gid=24983&lang=en
- Updated American Society of Clinical Oncology/Oncology Nursing Society chemotherapy administration safety standards including standards for the safe administration and management of oral chemotherapy. J Oncol Pract. 2013;9(2 Suppl):5s-13s.
- [Google Scholar]
- A call to action for hazardous drug safety: Where we have been and where we are now. Clin J Oncol Nurs. 2016;20:20-4AP.
- [Google Scholar]
- Voices of hope from rural Rwanda: Three oncology nurse leaders emerge. Oncol Nurs Forum. 2016;43:661-4.
- [Google Scholar]
- Silent saviours: Family members in a Bangladeshi hospital. Anthropol Med. 2013;20:278-87.
- [Google Scholar]
- 2013. Ward Boys in Gujarat, India: Doing Much More Than Meets the Eye Exploring Global Health Issues Through Sustainability and Education, Salt Lake City, UT. Available from: http://www.studentglobalhealthinitiative.web.utah.edu/archived-events/new-page/conference-abstracts/ward-boys-in-gujarat-india-doing-much-more-than-meets-the-eye
- 2013/2014. Teaching the Ward Boys in Gujarat, India. Illuminations: The Magazine for the University of Utah School of Medicine Alumni and Friends. :11. Available from: http://www.medicine.utah.edu/alumni/images/REVISEDREPOSTfinal214_links.pdf
- The role of the clinical nurse specialist in promoting evidence-based practice and effecting positive patient outcomes. J Contin Educ Nurs. 2007;38:262-70.
- [Google Scholar]
- 2016. International Society of Nurses in Cancer Care (ISNCC). Strengthening the Oncology Nursing Workforce in Low- and Middle -Income Countries to Address the Growing Cancer Burden, White Paper. Available from: http://www.c.ymcdn.com/sites/www.isncc.org/resource/resmgr/publications/White_Paper_Final_Revisions_.pdf
- Nurses’ ethical reasoning and behaviour: A literature review. Int J Nurs Stud. 2010;47:635-50.
- [Google Scholar]
- Oncology nursing workforce capacity building in rural Rwanda: Strengthening specialized cancer care through nursing education and skill development. Ann Glob Health. 2016;82:484.
- [Google Scholar]
- Introduction of palliative care into undergraduate medical and nursing education in India: A critical evaluation. Indian J Palliat Care. 2004;10:55.
- [Google Scholar]
- 2013. Europeoan Oncology Nursing Society (EONS) Cancer Nursing Curriculum. Available from: http://www.cancernurse.eu/education/eons_cancer_nursing_curriculum.html
- 2016. Oncology Nursing Society (ONS). Chemotherapy/Biotherapy Certification Course. Available from: https://www.ons.org/content/onsoncc-chemotherapy-biotherapy-certificate-course
- 2016. End of Life Nursing Education Consortium (ELNEC), International. Available from: http://www.aacn.nche.edu/elnec/about/elnec-international
- 2016. The Australian Government Department of Health. Palliative Care Curriculum for Undergraduates. Available from: http://www.pcc4u.org
- Educational needs and strategies of pediatric oncology nurses in low- and middle-income countries. An International Society of Pediatric Oncology- Pediatric Oncology in Developing Countries Nursing Working Group Initiative. Cancer Nurs. 2014;37:E36-47.
- [Google Scholar]
- The Global Opioid Policy Initiative (GOPI) project to evaluate the availability and accessibility of opioids for the management of cancer pain in Africa, Asia, Latin America and the Caribbean, and the Middle East: Introduction and methodology. Ann Oncol. 2013;24(Suppl 11):xi7-13.
- [Google Scholar]
- Next steps in access and availability of opioids for the treatment of cancer pain: Reaching the tipping point? Ann Oncol. 2013;24(Suppl 11):xi60-4.
- [Google Scholar]
- Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in Asia: A report from the Global Opioid Policy Initiative (GOPI) Ann Oncol. 2013;24(Suppl 11):xi24-32.
- [Google Scholar]
- Examining influences on the availability of and access to opioids for pain management and palliative care. J Pain Palliat Care Pharmacother. 2013;27:255-60.
- [Google Scholar]
- 2009. Human Rights Watch (HRW). Unbearable Pain: India's Obligation to Ensure Palliative Care. Available from: https://www.hrw.org/report/2009/10/28/unbearable-pain/indias-obligation-ensure-palliativecare
- Palliative care in India: Current progress and future needs. Indian J Palliat Care. 2012;18:149-54.
- [Google Scholar]
- A community partnership approach to building and empowering a palliative care resource nurse team. J Hosp Palliat Nurs. 2011;13:31-40.
- [Google Scholar]
- 2011. Government of India Ministry of Home Affairs, Office of the Registrar General and Census Commissioner, Census of India. Available from: http://www.censusindia.gov.in/Census_And_You/area_and_population.aspx
- Pain relief in the developing world: The experience of hospice Africa-Uganda. J Pain Palliat Care Pharmacother. 2003;17:107-18.
- [Google Scholar]
- Hospice and palliative care development in India: A multimethod review of services and experiences. J Pain Symptom Manage. 2008;35:583-93.
- [Google Scholar]
- Kerala, India: Status of cancer pain relief and palliative care. J Pain Symptom Manage. 2002;24:191-3.
- [Google Scholar]
- Critical ethnography, cultural safety, and international nursing research. Int J Qual Methods. 2010;9:240-51.
- [Google Scholar]
- Implementing a palliative care nurse leadership fellowship program in Uganda. Oncol Nurs Forum. 2016;43:395-8.
- [Google Scholar]
- A practical field guide to conducting nursing research in low- and middle-income countries. Nurs Outlook. 2015;63:462-73.
- [Google Scholar]
- Situational analysis of nursing education and work force in India. Nurs Outlook. 2013;61:129-36.
- [Google Scholar]
- Nurses’ workplace distress and ethical dilemmas in Tanzanian health care. Nurs Ethics. 2008;15:478-91.
- [Google Scholar]




