
Translate this page into:
Practice of Iranian Adolescents with Hemophilia in Prevention of Complications of Hemophilia
Address for correspondence: Dr. Fahimeh Alsadat Hosseini; E-mail: nurse_meds@sums.ac.ir
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Prerequisite for management of a chronic disease involves knowledge about its complications and their prevention. Hemophilia in adolescents influences all the aspects of their lives and thier performance.
Objectives:
The present study aimed to determine the performance of Iranian hemophilic adolescents in prevention of disease complications.
Patients and Methods:
In this descriptive-analytical study, 108 adolescents with hemophilia were selected through convenience sampling. Their performance in preventing the complications of hemophilia was evaluated by sending a semi-structured questionnaire to their addresses throughout Iran. Then, the data was analysed using the Statistical Package for Social Sciences (SPSS) software (v. 13) and descriptive and interferential statistics were used.
Results:
Overall, 32.1% of the participants controlled bleeding during the 1st hour. Inaccessibility of coagulation products was mainly responsible for inhibiting timely and proper bleeding control. In order to relieve bleeding associated pain, only 39.0% of the adolescents used analgesics. On the other hand, 19.8% of the subjects used nonpharmacological methods to relieve pain. The majority of the adolescents did not participate in sport activities (65.4%) others allocated less than 5 hours a week to physical activities (70.5%). In addition, the participants did not have favorable dietary patterns, exercise habits, and dental care. The results showed a significant relationship between the adolescents’ preventive practice with coagulation disorders and utilization of pharmacological pain relief methods. Also, significant relationships were found between severity of the disease; participating in physical activities, number of hours of physical activities; and disease complications.
Conclusions:
Iranian adolescents did not exhibit favorable practices towards complication prevention.
Keywords
Adolescents
Hemophilia
Prevention
Practice

INTRODUCTION
Hemophilia is an inherited coagulation disorder caused by a genetic defect of X-chromosome. It has a general prevalence of about one in every 10,000 people.[1] Hemophilia is traditionally classified as mild, moderate, and severe based on the level of coagulation factor in a person's blood compared to normal individuals.[2] Symptoms of hemophilia include hemarthrosis (especially in the knee, ankle, and elbow joints), soft-tissue hematomas, bruises, intraperitoneal bleeding, intracranial hemorrhage, and postoperative bleeding.[3] Recurrent hemarthrosis and soft-tissue hematomas can lead to acute arthropathy, contracture of the joints, and pseudotumors over time. These complications may, in turn, trigger chronic pain, inability, and decreased health-related quality of life.[34] Despite the extensive complications of hemophilia, appropriate treatment will provide patients with a chance of living a nearly normal life with high health-related quality of life.[5678]
Patients with hemophilia (particularly at moderate and severe levels) are often treated with prophylactic therapy to decrease both the duration and severity of bleeding.[9] Replacement of the missing clotting factors is an effective measure in treatment of the patients with hemophilia. However, 20–30% of the patients with hemophilia A and 5% of those with hemophilia B produce factor VIII and factor IX inhibitors, respectively. This will reduce the efficacy of alternative treatments,[10] lead to weaker prognosis, decrease quality of life, and increase treatment costs.[11] Viral infections related to transmission of blood products are other important complications that increase the possibility of cirrhosis, end-stage liver disease, and hepatocellular carcinoma.[12]
Due to high costs and inadequate specialized care, accessibility to replacement therapy in large scale is limited to developed countries. Unfortunately, such conditions are not available to the majority of patients in developing countries.[13] In the absence of proper treatment, patients with hemophilia (especially those with severe type of the disease) will experience clinical symptoms; including pain, swelling, and decreased joint range of motion (ROM) in early adolescence that affect their health and quality of life.[814] Therefore, hemophilia in developing countries is managed through options which do not require expensive therapeutic products.[15]
Control and management of a chronic disease entailidentifying and preventing its complications.[16] Yet, almost 50% of adolescents with chronic diseases do not completely adhere to therapeutic recommendations.[16] As patients with hemophilia experience various issues during their adolescence, which is undoubtedly a critical and important.[1718]
Previous studies have shown that high-quality informative and educational programs about causes of bleeding are essential for adolescents with hemophilia. Since adolescence is a stage of life full of questions and concerns about identity, self-confidence, and communications, controlling the disease in this period influences almost every aspect of an individual's life, including exercise, travelling, and others.[19] In Iran, the mean age of the patients with hemophilia was reported to be 25.92 ±15.19 years and half of the population was younger than 24 years. Hence, majority of the Iranian patients with hemophilia are adolescents.[20]
Educating adolescents in preventing complications of hemophilia will not only have remarkable economic benefits, but will also inhibit the unexpected complications due to the use of therapeutic products and enhance the patients’ quality of life. In 2002, Mohammad Zadeh et al., found that patients with hemophilia in Tehran (Iran) did not exhibit awareness, attitude, and complication prevention practices.[21] Although the complications of hemophilia result in numerous psychosocial outcomes, to the best of our knowledge, no previous study has evaluated these complications and their prevention methods. On the other hand, limited therapeutic resources in developing countries and ineffectiveness of the existing treatments because of increased inhibitor antibodies in some patients necessitate development of new efficient methods for reducing the disease complications in patients with hemophilia.
Considering the few related studies in Iran, the present study aims to determine the performance of the adolescents with hemophilia with regards to prevention of the disease complications. We hope to facilitate planning of possible future interventions.
PATIENTS AND METHODS
In this descriptive-analytical study, the target population included the adolescents with hemophilia whose names had been registered in Iranian centers for hemophilia. The study data were collected using a researcher-made questionnaire, consisting of items regarding the patients’ individual and social characteristics and their practice to prevent the complications of hemophilia. In this questionnaire, 30 items evaluated the adolescents’ preventive practice which included the following four dimensions: General preventive measures (12 items), dental care (five items), dietary pattern (five items), and physical activity (eight items). These items were responded based on a Likert scale with the following options: 1 (never), 2 (sometimes), and 3 (always). Thus, the total score of the questionnaire ranged from 30 to 90, with higher scores representing better preventive practices. The questionnaire's face and content validity as well as reliability were confirmed (Cronbach's alpha = 0.87). Considering the wide geographical distribution of the subjects, the questionnaires were mailed and completed through self-report. The process required cooperation of the authorities at local hemophilia institutes.
The patients aged 12 − 19 years who had coagulation disorder were included in the study if they were aware of their disease, were registered in the relevant hemophilia center, were willing to participate, and could answer questions. Using convenience sampling, 108 eligible patients were recruited into the study. After gaining the approval for the study from the Center of Health Policy Research and Hemophilia Center of Iran, coordination with hemophilia institutes throughout the country was carried out. The subjects were provided a thorough explanation about the research and were asked to fill out the questionnaires anonymously. They were ensured about the confidentiality of their information and their right to with draw from the study. Written informed consents for taking part in the study were also received from all the participants. Data collection lasted for 9 months (September 2011–May 2012). The obtained data were entered into the Statistical Package for Social Sciences (SPSS) statistical software, version 13.0 and were analyzed using frequency, mean, and standard deviation and analysis of variance (ANOVA), t-test, and Chi-square tests.
RESULTS
108 adolescents with hemophilia participated in the study and the data were collected from 11 hemophilia institutes across Iran. Majority of the participants were from East Azerbaijan Province. Male and female participants constituted 84.9% (n = 90) and 15.1% (n = 16) of the whole population, respectively. Most subjects (n = 42, 45.7%) were junior high school students. Moreover, 89.5% of the mothers were housewives and 46.8% of the fathers were self-employed [Table 1]. Disease-related characteristics of the participants have been presented in Table 2.


Results showed in 34 (32.1%), 18 (17.0%), 9 (8.5%), and 11 (10.4%) patients bleeding was controlled during the 1st hour, 1st–3rd hour, 3rd–6th hour, and after the 6th hour, respectively. Significant percentage of the patients (n = 34; 32.1%) were unaware of the duration of their bleeding control.
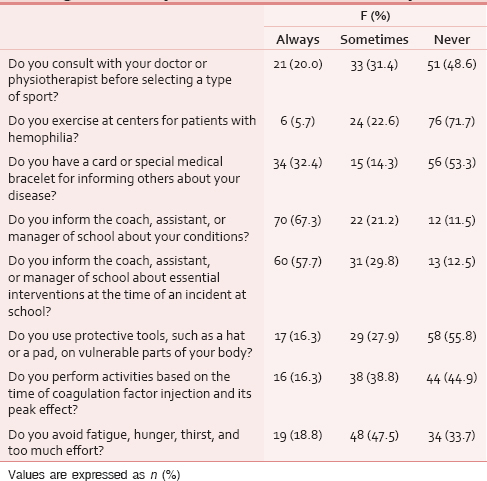
According to 44 subjects (47.8%), inaccessibility to coagulation factors or the required drugs at the time of incident was the most important factor that inhibited timely bleeding control. Others considered not taking the event leading to bleeding seriously (n = 21; 22.8%), not having sufficient information about the circumstances of necessary interventions at the time of bleeding (n = 15; 16.3%), and failing to identify the events leading to bleeding (n = 10; 10.9%) to be responsible for inappropriate bleeding control. However, two patients (2.2%) had no idea in this regard. The general preventive behaviors taken by the Iranian adolescents with hemophilia have been presented in Table 3.

Based on the results, only six adolescents (5.7%) did not use coagulation factors to control their disease. Among the 99 patients (94.3%) who used these factors, 46 (47.4%) received assistance from their family members, 37 (38.1%) received the coagulation factor by the help of a healthcare provider, 13 (13.4%) injected the factor themselves, and one (1.0%) used the coagulation factor by himself or with the help of a healthcare provider. The injections were made at home (n = 46; 46.5%), in the clinic (n = 37; 37.4%), either at home or in the clinic (n = 11; 11.1%), or in other places such as hospitals or treatment institutes (n = 5; 5.1%).
Majority of the participants (n = 64; 61.0%) did not use analgesics to relieve bleeding pain. Among the 44 patients (39.0%) who did, 25 (83.3%) used acetaminophen-codeine. Narcotics, corticosteroids, and even some nonsteroidal anti-inflammatory drugs were also used by other adolescents. Besides, about 85 patients (80.2%) mentioned that they did not use other techniques than drug therapy for controlling the pain arising from the disease. On the other hand, 21 participants (19.8%) stated that they used other techniques, with using ice compress being the most common one (n = 8; 44.4%).
Participation in sport activities was reported by only 37 subjects (34.6%) who were active in more than one sport (n=9; 26.5%), went swimming (n=6; 17.6%), played soccer (n=5; 14.7%), went body-building (n=4; 11.8%), played ping-pong (n=3; 8.8%), went cycling (n=2; 5.9%), and were involved in shooting, karate, volleyball, yoga, and walking (n=1 each). The majority of the adolescents (n = 43; 70.5%) did physical activities for 5hours a week or less. In addition, four patients (6.6%) exercised for about 5–10 hours a week, four (6.6%) had about 10–20 hours of weekly physical activity, and five (8.2%) had more than 20 hours of physical activity per week. However, four patients (6.6%) were not involved in any kind of physical or sport activities. Also, one subject (1.6%) did not know the exact time she/he devoted to sports [Table 4].
The results of the adolescents’ performance in relation to oral and dental care, dietary patterns, and overall preventive dimensions have been presented in Tables 5–7, respectively. Besides, the participants’ knowledge of various fields has been shown in Table 8. Accordingly, only 33 adolescents (32.4%) were aware of viral infections and their mean score of knowledge was 3.08 ±1.04.




The results indicated no significant relationships between the participants’ demographic characteristics and their preventive practice. However, the results of ANOVA demonstrated a significant relationship between coagulation disorders and the participants’ preventive practice mean scores (F = 2.95, degrees of freedom (df) =4, P = 0.03). Accordingly, the mean scores of the adolescents with hemophilia A (2.05 ±0.35) and hemophilia B (2.20 ±0.19) were higher compared to those of the adolescents affected by Von Willebrand (1.59 ±0.25). Also, the results of independent t-test showed a significant relationship between using pharmacological pain relief methods and the participants’ preventive practice scores (t =−2.36, df = 103, P = 0.02). The adolescents who did not use pharmacological pain relief methods (2.10 ±0.34) had better preventive practice in comparison to those who used these methods (1.94 ±0.3).
With respect to relationships among the categorical variables, results ofChi-square test revealeda significant relationship between sex and coagulation disorders (χ2 = 2 6.84, df = 4, P = 0.0001). Accordingly, all the adolescents with hemophilia A and B were male; in this regard female adolescents had milder coagulation disorders. The study results showed a significant relationship between the disease severity and the individual injecting the factor) χ2 = 23.07, df = 6, P = 0.001). Injection of coagulation factors was done by family members in the majority of the patients with moderate and severe disease, but by healthcare staff in those with mild disease. There was also a significant relationship between participating in physical activities and coagulation disorders (χ2 = 10, df = 4, P = 0.04). The ratio of the patients with hemophilia A who avoided physical activities to those who did such activities was 1.75. This ratio was higher compared to other coagulation disorders. Moreover, a significant relationship was found between the number of hours of doing physical activities and the disease complications (χ2 = 27.25, df = 15, P = 0.02). The participants who did physical activities for 5hours a week or less had morecomplications compared to the others. However, no significant relationships were observed between other disease-related characteristics and the patients’ preventive practice.
DISCUSSION
This study surveyed the practice of hemophilic adolescents in prevention of the complications of hemophilia. In this research, the majority of the participants was male and had severe hemophilia. Besides, a significant relationship was observed between gender and coagulation disorders and all the adolescents affected by hemophilia A and B were male, while female adolescents had milder coagulation disorders. Hemophilia usually affects men; thus, daughters of hemophilic men can be asymptomatic carriers of this disease.[22] In fact, a woman inherits hemophilia in case her father has hemophilia and her mother is a carrier of hemophilia, which is very rare.[22] In the present study, many of the subjects had received the coagulation factor since birth up to the age of 1 year. In severe and mild hemophilia, the disease symptoms are often demonstrated clearly and, consequently, the disorder is diagnosed in early life.[23] Because hemophilia has dramatic effects on social, economic, physical, and emotional life of hemophilic patients and their families[24] and its complications are serious and plentiful in severe type of the disease, measures are necessary to be taken to prevent the complications of this coagulation disorder.
In the current study, the commonest complications experienced by the patients were swelling and joint pain. From the viewpoint of the majority of the participants, pain was an almost persistent feeling which was sometimes combined with other complications. Physical condition of joints is considered as the best indicator of the efficacy of treatment modalities and the whole health system for patients with hemophilia.[25] Arthropathy is a clinical result of frequent hemarthrosis in patients with hemophilia, which in turn leads to pain, inability, and reduced quality of life.[26] Initiation of prophylaxis at early stages of life, when limited hemarthrosis has been experienced, will improve joint conditions. Hence, early prophylaxis is currently a standard treatment.[27] Zandian et al., studied 138 Iranian patients with hemophilia A and B and found the mean severity of arthropathy to be higher than that reported in similar studies performed in France and Spain. However, the mean annual use of factors VIII and IX was lower compared to other studies.[28] Unfortunately, lack of access to the required coagulation factors in Iran forces the health system to control hemarthrosis in patients with hemophilia only when necessary. In the present study also, more than half of the patients used coagulation factors only during bleeding. Treatment strategies for hemophilic arthropathy must focus on prevention of musculoskeletal complications arising from recurrent hemarthrosis.[26] Therefore, patients, especially adolescents, with hemophilia have to be provided with support to improve their practice towards effective prevention of different complications of their disease.
Few participants in our study were following a physiotherapy program. Physiotherapy helps maintain joint ROM and functionality, reduces swelling and pain, maintains the muscles strength, and prevents injuries.[13] After every coagulation factor injection, the patient has to adhere to an exercise program to enhance joint motion, reinforce progress, learn the correct method of walking, control pain, and perform physiotherapy at home.[29] Physiotherapy is also an essential part of the rehabilitation process in cases of severe joint injury and surgery. Preventive physiotherapy can strengthen the muscles around joints and improve motion, flexibility, and balance. A skilled physiotherapist can provide patients with recommendations regarding appropriate lifestyle and techniques to prevent and control bleeding and other musculoskeletal problems.[29] Apparently, as most of our subjects did not participate in a physiotherapy program, they were suffering from numerous disease complications. Since adolescence is a critical period in formation of a proper mental image, adolescent patients with hemophilia must be provided with facilities complementary to coagulation factor therapy (e.g., physiotherapy) to promote their health status and reduce the intensity of the disease complications.
More than two-third of the participants in this study did not have any knowledge regarding viral infections and others reported a little information about transmission routes and viral diseases’ symptoms. According to the previous researches, 67 and 78% of the adolescents with hemophilia did not have knowledge of viral transmission routes of hepatitis C and B, respectively.[16] Nowadays, many hemophilic patients are treated by coagulation factors prepared through recombination techniques or produced byplasma-derived factor concentrates through advanced viral inactivation method which decreases the threat of viral transmission. Nevertheless, there is a possibility of contamination with viral infections in consumers of blood products.[30] Therefore, planning to improve the knowledge of viral disorders has a vital impact on prevention of some related complications.
Only about one third of the participants in the current study controlled bleeding during its first hour. The most important obstacles against proper and timely interventions to control bleeding were inaccessibility to coagulation factors or other required drugs at the time of the incident and not taking the event leading to bleeding seriously. According to the National Hemophilia Foundation and the Centers for Disease Control and Prevention in the USA; more than two-third of the adolescents with hemophilia failed to control bleeding during its 1st hour due to inappropriate diagnosis and treatment of bleeding.[16] The relative contradiction between the results of the current study and those of the previous researches about the obstacles against timely management of bleeding might be attributed to differences in the existing facilities for hemophilic patients (particularly accessibility to coagulation products) in developing and developed countries. In cases of impracticability or inappropriateness of prophylaxis as a standard care in hemophilic patients (limitation of sources and possibilities),[313233] bleedings which require treatment must be treated as soon as possible.[34] Quick treatment is of utmost importance since the skeletal system of an adolescent person is very sensitive to complications of hemophilia and severe structural defects may develop quickly.[13] Prevention of bleeding events through timely treatment inhibits hyperemia in joints as well as the subsequent inflammation and potential hemophilic arthropathy. The treatment should continue until the complication is alleviated and joint ROM and muscular strength are enhanced as much as possible.[13] Our participants used coagulation products to treat their bleeding. However, besides accessibility to coagulation factors, patients with hemophilia require comprehensive knowledge about the symptoms of bleeding and the importance of using coagulation factors soon after bleeding or even when they doubt bleeding.
In the current study, majority of the families administered coagulation factor. Additionally, a significant relationship was found between the disease severity and the individual injecting the factor. Injection of coagulation factors was done by family members in majority of patients with moderate and severe types of disease and by healthcare staff in those with mild disease. With hemophilia being a chronic disease and treatment centers being inaccessible, independent injections by patients or their families are necessary to prevent the complications of the disease. Complementary educations to update patients’ knowledge and periodical control of their practice are thus critical.
Most adolescents in the present study did not keep ice bags in the freezers of their houses or in their bags. They also had poor performance in reporting high fever when using intravenous injection tools, keeping the injured limb above the heart level, relieving pain using warm compress, and referring to related institutes to get information about the successful treatment process. Moreover, they only sometimes performed other preventive behaviors, such as keeping the injured limb motionless at the time of bleeding, using appropriate cover for ice, and frequent inspection of motion of their joints. Since the mentioned interventions have a major role in controlling the complications of hemophilia, poor performance of the patients might have been caused by their unawareness of and inattention to the preventive interventions. The findings of the current study revealed a significant relationship between coagulation disorders and the participants’ mean score of preventive practice. Accordingly, the mean scores of the adolescents with hemophilia A and B were higher than those of the adolescents affected by Von Wille brand. This is probably due to the fact that the adolescents with serous kinds of coagulation disorders have better preventive practice to avoid the unpleasant complications of their disorder.
More than half of the participants in this study did not use analgesics to relieve pain. Drugs, such as acetaminophen, can be effective in controlling or relieving pain. Yet, it must be considered that most analgesics available in drug stores contain compounds of acetylsalicylic acid (ASA), that is, the active element of aspirin; while the individuals with hemophilia must avoid products which contain aspirin. Aspirin prevents clot formation and clumping of platelets and may hence aggravate bleeding in hemophilic patients. Other analgesics, such as Advil and ibuprofen, may also worsen bleeding through disturbing the function of platelets.[35] Safer options include paracetamol, acetaminophen, and milder analgesic narcotics;[13] and the patients must be provided with the necessary training in this regard.
Less than one-fourth of our participants used techniques other than drugs to control their pain. Lack of movement may not be necessary for patients with mild hemarthrosis. RICE strategy (rest, ice, compression, and elevation) can also be useful in pain relief.[36] Ice bags can be used for 20 min every 4–6 hours until pain is relieved. Protection of joints by splints, slings, or compression bandages can be beneficial, too. After bleedings in extremities, patients have to rest in bed for 1 day, elevate the limb while sitting for 3–4 days, avoid imposing weight, and use a crutch or a wheelchair at the time of walking.[36] As bleeding control relieves pain, after coagulation factor injection, patients with hemophilia need to benefit from some sort of nonpharmacological techniques, such as rest, ice, compression, and elevation of limb, to effectively relieve pain and prevent its complications. Since hemophilia is a chronic disease with recurrent pain that influences the patients’ mental and physical conditions, such nonpharmacological methods can be safe, cheap, and accessible options to treat pain. On the other hand, most adolescents in the current study did not use drugs to relieve pain resulting from bleedings and these participants had better preventive practice in comparison to the others who used pharmacological methods of pain relief. Therefore, improving the patients’ well-being and quality of life requires informing them about the importance of nonpharmacological pain relief methods.
A small proportion of our participants were involved in sport activities and many of them played more than one sport (particularly swimming and soccer). Similarly, Fromme et al., found that 88.6% of the adolescents participated in one or more sport fields for fun. They reported swimming, tennis, and soccer as the most common sports. Moreover, adolescent and adult patients in their study considered entertainment and social aspects to be more important than the health aspect in selecting a sport.[37] The majority of the participants in our study were involved in physical activities for at most 5hours a week. Besides, the participants who were active for 5 hours or less a week had significantly higher complications compared to the others. In addition to general effects on metabolism and the cardiovascular system, physical activity can reduce the complications of hemophilia through muscle strengthening, which in turn improves the condition of the joints and finally decreases the complications of bleeding.[37] Based on a research by National Hemophilia Foundation in the USA and the Centers for Disease Control and Prevention, 60.0% of the patients with hemophilia avoided or had limited physical activity to prevent or decrease the complications of hemophilia.[16] Furthermore, the present study findings indicated a significant relationship between participating in physical activities and coagulation disorders. Accordingly, the number of patients with hemophilia A who avoided physical activities was considerably higher than those who participated in such activities. Although a significant number of respondents in the study by Fromme et al., played ball sports,[37] the research results demonstrated vulnerability risk in ball sports to be one in 5.5 individuals.[38] According to Fromme et al., most adolescents were interested in high risk activities, such as soccer.[37] Nonetheless, patients with hemophilia are recommended to participate in safe sport programs and proper exercises to promote their physical functionality.[39] As a result of such recommendations, there is a high rate of quitting sport activities among these patients.[40] A sport will be practiced regularly by patients only if it is viewed as fun and has a positive image among their healthy peers.[41] Hence, activities for patients with hemophilia have to be selected in collaboration with specific care centers and the responsible physician by taking every individual's conditions and interests into account.
Our participants did not have appropriate behaviors in consulting with their physicians or physiotherapists before selecting a sport, having a card or special medical bracelet for informing others about their disease, performing activities when the coagulation factor has the highest effect, using protective tools such as a hat or a pad on vulnerable parts of the body, and doing exercises in centers for patients with hemophilia. The adolescents stated that they did not attend centers for hemophilic patients probably due to absence of consulting centers to inform patients about appropriate sports based on their individual conditions. Yet, centers providing sport services under supervision of hemophilia treatment centers can be effective in prevention and control of disease complications.
Generally, participants of the present study had favorable performance in oral and dental care. Most of the adolescents, were not referred to the dentists collaborating with hemophilia centers. This might have been due to inaccessibility to these centers or unawareness about the existence of such centers. Ina recent study, Alpkilic et al., reported that the prevalence of brushing was significantly higher in the healthy control population than in the patients with hemophilia.[42] In addition, Saxena and Shashikiran found that the prevalence of dental caries was 87.19% among 11–15-year-old patients and suggested dental treatment to be necessary for these patients. Hence, dentistry services are required to prevent oral diseases in hemophilic patients.[43] Furthermore, Alpkilic et al., concluded that management and control of oral diseases in patients with hemophilia should start from childhood. As parents play a major role in the care provided for children, they must also receive recommendations about the importance and necessity of oral care.[44]
Our study participants did not follow an appropriate dietary pattern. They did not avoid stimulating and spicy foods, use laxatives incase of constipation, and prevent fatness. Shunning stimulating foods and inhibiting constipation can help prevent bleeding in the digestive system of patients with hemophilia. In addition, a diet rich in iron can compensate for the deficiency of some necessary nutrients in the hematopoiesis process. Considering the lower rate of physical activity among these patients compared to the healthy population, their diet must keep their proper weight and prevent osteoporosis.
The limitations of this study included problems resulting from insufficient facilities in some hemophilia institutes, impossibility of communication and coordination with some institutes, some institutes’ inaccessibility to adolescents because of patient referral system in some provinces, lower population of adolescents with hemophilia than other age groups in the country, unwillingness to cooperate, and not returning the questionnaires. Despite the frequent efforts in order to cooperate with hemophilia institutes throughout the country, only 11 institutes cooperated in this research. Other study limitations were inaccuracy of the participants in answering the questionnaire items due to fatigue or disease-related conditions and the small sample size, especially in different categories of coagulation disorders.
CONCLUSIONs
The results of the present study demonstrated that Iranian adolescents with hemophilia did not exhibit favorable practice in some fields of prevention of disease complications. Therefore, such patients should be provided with adequate information to prevent the lifelong and fatal complications of the disease. Appropriate management and control of hemophilia is a key factor in decreasing and preventing long-term problems which cause high disease management costs. When resources and possibilities are limited, education is the cornerstone of hemophilia care.[45] Even with limited number of coagulation products, it is possible to improve hemophilic patients’ lives in developing countries through education, prevention, and complementary cares. National associations of hemophilia in developing countries play an important role in increasing awareness, education, and supporting the families of the patients with hemophilia.[15] Nevertheless, preventing the disease complications in adolescents cannot be possible without solid planning, provision of necessary facilities, collaboration of several medical and educational teams, and considering the patients’ individual characteristics. Moreover, patients’ knowledge and practice must be evaluated periodically. In necessary cases, interventions should also be carried out to improve such patients’ well-being and quality of life. Such interventions cannot only decrease the heavy load of treatment costs, disabilities, and lifelong physical and mental hemophilia complications, but they can also optimize the allocation of national budget.
ACKNOWLEDGMENT
This study was extracted from a research project approved by the Health Policy Research Center of Shiraz University of Medical Sciences, Shiraz, Iran. Hereby, the authors would like to thank the honorable authorities of the centers under study, Ms Tabaghchi, Mr Hashemi, and Dr Ziaey, and the officials of hemophilia centers around Iran. They are also grateful for the adolescents who participated in this study. Also thankful to Ms A Keivanshekouh at the Research Improvement Center of Shiraz University of Medical Sciences for improving the use of English in the manuscript.
Source of Support: This study was supported by the Health Policy Research Center of Shiraz University of Medical Sciences, Shiraz, Iran.
Conflict of Interest: None declared.
REFERENCES
- Mild hemophilia. 2006. Treatment of Hemophilia Monographs No. 41, December 2006. Montreal: World Federation of Hemophilia; Available from: http://www.wfh. org/2/docs/Publications/Diagnosis_and_Treatment/TOH.41_ Mild.Hemophilia.pdf
- [Google Scholar]
- Factor VIII and Factor IX Subcommittee. Recommendation of the scientific subcommittee on factor VIII and factor IX of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost. 2001;85:560.
- [Google Scholar]
- Hereditary plasma clotting factor disorders and their management. 2008. Treatment of Hemophilia Monographs No. 4, April 2008. Montreal: World Federation of Hemophilia; Available from: http://www.wfh.org/2/docs/Publications/Diagnosis_and_Treatment/TOH-4-Hereditary
- [Google Scholar]
- Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. 2007;357:535-44.
- [Google Scholar]
- Co-morbidities and quality of life in elderly persons with haemophilia. Br J Haematol. 2009;148:522-33.
- [Google Scholar]
- The aging patient with hemophilia: Complications, comorbidities, and management issues. Hematology 2010:191-6.
- [Google Scholar]
- Bone density and health-related quality of life in adult patients with severe haemophilia. Haemophilia. 2011;17:304-11.
- [Google Scholar]
- Joint outcomes in patients with haemophilia: The importance of adherence to preventive regimens. Haemophilia. 2009;15:1219-27.
- [Google Scholar]
- Inhibitor treatment in haemophilias A and B: Summary statement for the 2006 international consensus conference. Haemophilia. 2006;12:1-7.
- [Google Scholar]
- Assessing risk factors: Prevention of inhibitors in haemophilia. Haemophilia. 2010;16:10-5.
- [Google Scholar]
- End-stage liver disease in persons with hemophilia and transfusion-associated infections. Blood. 2002;100:1584-9.
- [Google Scholar]
- Haemophilia and joint disease: Pathophysiology, evaluation, and management. J Comorbidity. 2011;1:51-9.
- [Google Scholar]
- Association of Hemophilia Clinic Directors of Canada and Canadian Association of Nurses in Hemophilia Care. A survey of factor prophylaxis in the Canadian haemophilia A population. Haemophilia. 2004;10:679-83.
- [Google Scholar]
- Treatment options in the management of hemophilia in developing countries. the World Federation of Hemophilia (WFH). DECEMBER 2005 NO 37. Available from: http://www1.wfh.org/2/docs/Publications/Diagnosis_and_Treatment/TOH37_Treatment_Dev_Countries_Add.pdf
- [Google Scholar]
- Knowledge, attitudes, and behaviors of youths in the US hemophilia population: Results of a national survey. Am J Public Health. 2006;96:1618-22.
- [Google Scholar]
- Assessment of hemophilia patients’ knowledge about self- care method. MSC thesis. Tehran: Tarbiat Modarres University; 1989.
- [Google Scholar]
- Assessment of the effect of self-care on quality of life in patients with liver cirrhosis inpatient in hospitals of Tehran. MSC thesis. Tehran: Tarbiat Modarres University; 2002.
- [Google Scholar]
- The effect of self care program on quality of life in hemophilic adolescent. Monthly J Med Daneshwar, Shahed university 2007:14.
- [Google Scholar]
- Occurance of hemophilia in IRAN. 13th Congress of the European Hematology Association, June 12-15, 2008. 2008. Haematologica. 93:553. Abs. 1465. Available from: http://online.haematologica.org/EHA13/browserecord.php?-action=browse and -recid=3018
- [Google Scholar]
- Assessment of knowledge, attitude and performance of hemophilic patient on hemophilia disease. Annals of Research activities of Rehabilitation Faculty of shahid Beheshti University of Medical Sciences in 2002-2003. Available from: http://old.sbmu.ac.ir/rehabilitation/Boltan%2081.82%20Newone.doc
- [Google Scholar]
- World Federation of Hemophilia. Carriers and women with hemophilia. In W.F.O. Hemophilia ed. World Federation of Hemophilia. 2012. Québec, Canda: World Federation of Hemophilia; Available from: http://www1.wfh.org/publications/files/pdf-1471.pdf
- [Google Scholar]
- The Swedish Haemophilia Society. Swedish guidelines for: The care and treatment of hemophiliacs. The haemophilia centres in Malmö, Gothenburg and Stockholm 2003
- [Google Scholar]
- Living with haemophilia and Von Willebrand's: A descriptive qualitative study. Patient Educ Couns. 2007;68:235-42.
- [Google Scholar]
- Joint evaluation instruments in hemophilia. In: Rodriguez-Merchan EC, ed. The Hemophilic Joints. Oxford: Blackwell Publishing; 2003. p. :45-55.
- [Google Scholar]
- Hemophilia Clinical Consults: Hemophilic Arthropathy, Reduced Bone Density, and Preventive Strategies. Clinical Consults. June 17, 2011. Available from: http://www.bloodcmecenter.org/Downloads/Hemophilic_Arthropathy.pdf
- [Google Scholar]
- Assessment of prevalence and severity of artropathy in the hemophilic patients referred to hemophilia center of Shafa Hospital. Med Sci J 2008:7.
- [Google Scholar]
- Articular bleeding (hemarthrosis) in hemophilia. An orthopedist's point of view. 2008. Treatment of Hemophilia Monographs No. 23, April. 2008. Montreal: World Federation of Hemophilia; Available from: http://www.wfh.org/2/docs/Publications/Musculoskeletal_Physiotherapy/TOH-23-Hermarthrosis-Revised2008.pdf
- [Google Scholar]
- The epidemiology of virus transmission by plasma derivatives: Clinical studies verifying the lack of transmission of hepatitis B and C viruses and HIV type 1. Transfusion. 1999;39:1160-8.
- [Google Scholar]
- Practice patterns in haemophilia A therapy—a survey of treatment centres in the United States. Haemophilia. 2003;9:549-54.
- [Google Scholar]
- Consensus perspectives on prophylactic therapy for haemophilia: Summary statement. Haemophilia. 2003;9:1-4.
- [Google Scholar]
- Why is primary prophylaxis underutilized in the United States? Haemophilia. 2003;9:670-2.
- [Google Scholar]
- A Guide for Families: Complications of hemophilia, Part 3- pain in hemophilia. P 20. Available from: http://www.hemophilia.ca/files/Chapter%2008.pdf
- [Google Scholar]
- World Federation of Hemophilia. Guidelines for the management of hemophilia. 2005. Montreal: World Federation of Hemophilia; Available from: http://www.wfh.org/2/docs/Publications/Diagnosis_ and_Treatment/Guidelines_Mng_Hemophilia.pdf
- [Google Scholar]
- Participation in sports and physical activity of haemophilia patients. Haemophilia. 2007;13:323-7.
- [Google Scholar]
- The number of accidents in school sports in general lowers Schools in Westphalia-Lippe. (1st Ed). Mu nster: Municipality Unfallversicherungsverband Westfalen-Lippe; 1991.
- [Google Scholar]
- Physical training increases isometric muscular strength and proprioceptive performance in haemophilic subjects. Haemophilia. 2003;9:86-93.
- [Google Scholar]
- Behavioral treatment of adherence to therapeutic exercise by children with hemophilia. Arch Phys Med Rehabil. 1987;68:846-9.
- [Google Scholar]
- Sports and hemophilia: Antagonist or protagonist. Clin Orthop Relat Res. 1996;328:25-30.
- [Google Scholar]
- Oral and general health related quality of life among young haemophilia patients. Haemophilia. 2009;15:193-8.
- [Google Scholar]
- Prevalence of dental caries and treatment needs among hemophilic children of Kota city. RAJASTHAN. Annals and Essences of Dentistry. 2010. II Available from: http://www.aedj.in/images/9/94/2.2.18-21.pdf
- [Google Scholar]
- Dental and Periodontal Health in Children with Hemophilia. JOURNAL OF COAGULATION DISORDERS. JCD 2009; 000: (000). Month 2009. 1-4. Available from: http://www.slm.hematology.com/uploads/media/jcd199794_Dental_and_Periodontal_Health_in_Children_with_Hemophilia.pdf
- [Google Scholar]
- Costs of care in hemophilia and possible implications of health care reform. Hematology 2011:413-8.
- [Google Scholar]




