
Translate this page into:
Trajectories of Depression, Anxiety, and Stress among Breast Cancer Patients: Assessment at 1st Year of Diagnosis
*Corresponding author: Jyoti Srivastava, Department of Psychology, Veerangna Maharani Laxmibai Government Girls Degree College, Bundelkhand University, Jhansi, Uttar Pradesh, India. jyotisrivbhu@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Srivastava J, Shukla HS. Trajectories of Depression, Anxiety, and Stress among Breast Cancer Patients: Assessment at 1st Year of Diagnosis. Indian J Palliat Care. doi: 10.25259/IJPC_219_2023
Abstract
Objectives
Breast cancer is a life-altering diagnosis that can significantly impact the mental health of patients. Understanding the trajectories of psychological symptoms is crucial for providing effective support and interventions. This empirical research paper aims to investigate the longitudinal trajectories of depression, anxiety, and stress among breast cancer patients within the first year of diagnosis.
Materials and Methods
A longitudinal study design was employed to assess depression, anxiety, and stress levels at four-time points: baseline (diagnosis), 3 months, 6 months, and 12 months after diagnosis. The participants included breast cancer patients (n = 200) recruited fro m the outpatient as well as inpatient department of Surgical Oncology, Sir Sunderlal Hospital, Banaras Hindu University, Varanasi, India. The Depression, Anxiety, and Stress Scale-21 was administered to measure psychological symptoms. Trajectories of depression, anxiety, and stress were analysed using mixed-effects modelling.
Results
The results indicated varying trajectories of depression, anxiety, and stress during the 1st year of diagnosis. At baseline, participants reported significantly higher levels of depression (Mean [M] = 16.42, standard deviation [SD] = 4.89), anxiety (M = 14.36, SD = 5.22), and stress (M = 18.58, SD = 5.72) compared to the general population norms. Over the 12 months, depression levels gradually decreased (β = −0.28, P < 0.001), anxiety levels remained relatively stable (β = −0.15, P < 0.05), while stress levels showed a significant decrease (β = −0.14, P < 0.05).
Conclusion
The findings suggest that breast cancer patients experience distinct trajectories of psychological symptoms during the 1st year of diagnosis. While depression showed a gradual decline, anxiety remained relatively stable, and stress exhibited a significant decrease. These results indicate the importance of addressing psychological well-being throughout the cancer journey, as patients may face different emotional challenges at various stages.
Keywords
Anxiety
Breast cancer
Depression
Longitudinal study
Stress

INTRODUCTION
Breast cancer remains a significant global health concern, affecting millions of women annually and presenting multifaceted challenges beyond the physical aspects of the disease. Psychosocial well-being plays a pivotal role in the cancer journey, influencing patients’ ability to cope with the diagnosis, treatment, and subsequent life adjustments.[1] As such, understanding the trajectories of psychological outcomes, such as depression, anxiety, and stress, among breast cancer patients is of paramount importance.[2] Previous research has illuminated the dynamic nature of these psychological responses, revealing diverse patterns of change over time.[3,4] However, there remains a need to delve deeper into the nuances of these trajectories to inform targeted interventions. Moreover, the role of individual characteristics, such as age, in moderating these trajectories has garnered growing interest, given its potential to guide personalised supportive strategies.[5,6] Younger patients, for instance, might experience more profound changes in psychological symptoms compared to their older counterparts. However, the role of age as a moderator in shaping the trajectories of psychological distress among breast cancer patients remains an area requiring further investigation. This study aims to contribute to the existing literature by examining the trajectories of depression, anxiety, and stress among breast cancer patients during the critical 1st year following diagnosis, adopting a longitudinal design to assess breast cancer patients’ psychological well-being at multiple time points during their initial year of diagnosis while also considering the potential moderating effects of age. In addition, the study explores the potential moderating effect of age on these trajectories. This research contributes to the nuanced understanding of psychological responses in breast cancer patients, facilitating the development of targeted interventions to optimise patients’ well-being during this critical phase. The insights garnered from this investigation hold promise for informing the development of tailored psychosocial interventions that align with the unique needs of patients at different stages of their cancer journey. Ultimately, our findings will inform the development of effective interventions to improve patients’ mental health outcomes and overall well-being during their challenging journey with breast cancer.
MATERIALS AND METHODS
Sample
The sample for this empirical research article consisted of 200 breast cancer patients who were recruited from the Department of Surgical Oncology, Sir Sundarlal Hospital, Banaras Hindu University, Varanasi, India. The participants were selected based on specific inclusion and exclusion criteria to ensure a representative and homogenous sample while minimizing potential confounding factors. Only those patients were included in the study who had to have received a confirmed diagnosis of breast cancer within the past 3 months, aged 18 years or older, currently undergoing active treatment for breast cancer, or had recently completed primary treatment. Individuals with a history of pre-existing psychological disorders or chronic mental health conditions, such as depression or anxiety disorders, or with pre-existing chronic illnesses unrelated to breast cancer were excluded from the study. As a part of the PhD research study, the protocol of the research was in accordance with ethical standards and was approved by the Institution’s Ethics committee (Reference No.-ECR/Bhu/Inst/UP/2013/Re-registration2017dt.31.01.2017/ No.Dean/2017/EC/24.10.2017) that the final sample consisted of 200 participants from Sir Sundarlal Hospital, Banaras Hindu University, Varanasi, India.
Measures
Depression, anxiety and Stress Scale 21 (DASS-21)
The DASS-21 is a widely used self-report questionnaire designed to assess the severity of symptoms related to depression, anxiety, and stress.[7] The scale comprises 21 items, with 7 items dedicated to each of the three subscales: depression, anxiety, and stress. Participants rate the frequency and intensity of their experiences over the past week on a 4-point Likert scale, ranging from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). Higher scores on each subscale indicate more severe symptoms of depression, anxiety, or stress. The DASS-21 is a reliable and valid tool commonly employed in research and clinical settings to measure psychological distress among diverse populations, including breast cancer patients. The internal reliabilities of the anxiety (α = 0.83), depression (α = 0.85), and stress (α = 0.80) scales in the present study were good. The Hindi adaptation of the scale also holds good psychometric properties.[8]
Perceived social support (PSS)
Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India Social Support Questionnaire (PGI SSQ) was administered to assess PSS.[9] Out of the 18 items, seven are positively worded, and 11 are negatively worded. Each item is scored on 5 5-point scale from “fully” to “not at all,” with a high score reflecting greater social support. The Hindi adaptation of the PGI SSQ achieves good reliability and validity among the Indian Population. The Cronbach’s alpha was found to be 0.67 for the present sample.[10-12]
Breast cancer treatment and progression data
Medical records were utilised to gather information about participants’ breast cancer diagnosis, treatment regimens and disease progression. Relevant medical data included cancer stage at diagnosis, tumour characteristics, treatment modalities (e.g. surgery, chemotherapy and radiation therapy), hormone receptor status and treatment adherence. This data provided essential clinical context for understanding the potential impact of cancer-related factors on distress trajectories.
Demographic and clinical questionnaire
Participants completed a demographic and clinical questionnaire, providing information about their age, ethnicity, education level, marital status, employment status, and other relevant socio-demographic factors. In addition, the questionnaire inquired about their previous history of mental health conditions and chronic illnesses unrelated to breast cancer. This information helped characterise the sample and control for potential confounding variables that could influence distress levels.
The DASS-21 served as the primary tool to measure psychological distress, while other measures provided valuable contextual information, health-related quality-of-life assessments, and cross-validation to ensure the robustness and accuracy of the study’s findings.
Procedure
Participants completed the DASS-21 at 4 time points: baseline (within 1 month of diagnosis, T1), 3 months after diagnosis (T2), 6 months after diagnosis (T3), and 12 months after diagnosis (T4).
Statistical analysis
Descriptive statistics were computed to summarise the characteristics of the sample and the levels of depression, anxiety, and stress at each time point. Latent growth curve modelling (LGCM) was used to identify trajectories of depression, anxiety, and stress over the 1st year following a breast cancer diagnosis. LGCM allowed for the examination of individual variability in initial levels and rates of change in psychological symptoms over time. Covariates (e.g., age, socioeconomic status, treatment modality, and social support) were included in the LGCM models to assess their associations with the trajectories of depression, anxiety, and stress. Each covariate was regressed onto the intercept and slope parameters to examine its influence on initial levels and changes in psychological symptoms. Post hoc assessment was also conducted to compare trajectory groups and examine differences in symptom severity and change patterns between the identified trajectory groups. Statistical analyses were performed using SPSS-21 software developed by IBM.
RESULTS
Demographic characteristics
The mean age of the participants was 52.3 years (standard deviation [SD] = 8.6). The distribution of cancer stages among the participants was as follows: Stage I (n = 75, 37.5%), Stage II (n = 85, 42.5%), Stage III (n = 30, 15%) and Stage IV (n = 10, 5%). The education level of the participants varied, with 30% having completed high school, 50% having some college education, and 20% having a bachelor’s degree or higher [Table 1].
| Variables | n=200 (%) |
|---|---|
| Age (in years) | |
| 30–49 | 136 (68) |
| 50–59 | 42 (21) |
| 60+ | 22 (11) |
| Education | |
| Up to high school | 59 (29.5) |
| Intermediate | 78 (39) |
| Graduate and above | 63 (31.5) |
| Marriage | |
| Married | 178 (89) |
| Single/widow/divorcee | 22 (11) |
| Residence | |
| Rural | 122 (61) |
| Urban | 60 (30) |
| Semi-urban | 18 (09) |
| Family income (per month) | |
| Up to 20000/-INR (Indian Rupee) | 150 (75) |
| >20000/- INR | 48 (24) |
| Family type | |
| Nuclear | 76 (38) |
| Joint | 124 (62) |
| Employment | |
| Housewife | 146 (73) |
| Self-employed | 36 (18) |
| Government/private employee | 18 (9) |
| Stage of disease | |
| I | 75 (37.5) |
| II | 85 (42.5) |
| III | 30 (15) |
| IV | 10 (5) |
Descriptive statistics (Mean and SD) were performed to assess the mean of self-reported accounts DASS and PSS. The estimated means for each psychological outcome at baseline (time of diagnosis) and at the 3-month, 6-month, and 12-month follow-up assessments are displayed in Table 2.
| Time point | Depression (M±SD) | Anxiety (M±SD) | Stress (M±SD) |
|---|---|---|---|
| Baseline (T1) | 16.42±4.9 | 14.36±5.2 | 18.6±5.7 |
| 3 months (T2) | 13.9±4.2 | 12.4±3.8 | 15.2±3.9 |
| 6 months (T3) | 13.5±4.1 | 11.9±3.8 | 14.8±4.0 |
| 12 months (T4) | 12.7±4.0 | 11.1±3.7 | 14.1±3.9 |
SD: Standard deviation, M: Mean
Model analysis
The mixed-effects models were used to analyse the trajectories of depression, anxiety and stress levels over the 1st year following breast cancer diagnosis. The statistical analysis revealed significant main effects of time on depression, anxiety, and stress levels using repeated measures analysis of variance. There were significant differences in depression (F(3, 198) = 12.72, P < 0.001), anxiety (F(3, 198) = 10.21, P < 0.001), and stress (F(3, 198) = 8.93, P < 0.001) levels across the 4 time points (baseline, 3 months, 6 months and 12 months) following breast cancer diagnosis. The mixed-effects models revealed significant variation among participants in baseline depression (σ2 = 4.78, P < 0.001), anxiety (σ2 = 3.62, P < 0.001), and stress (σ2 = 5.12, P < 0.001) levels. This indicates that participants entered the study with different baseline psychological profiles. The individual differences in baseline scores may have contributed to the distinct trajectories observed in the longitudinal analysis.
Longitudinal trajectories
Using LGCM, participants were classified into three trajectories based on their depression, anxiety, and stress scores over time: (1) stable, (2) improving, and (3) worsening.
Trajectories of depression
Stable Trajectory: Participants whose scores did not deviate by more than ±1 SD from their baseline values over time. This group (n = 70, 35%) exhibited stable depression levels over the 1st year following breast cancer diagnosis. Their depression scores remained relatively constant throughout the study period, suggesting minimal changes in psychological symptoms [Figure 1a].
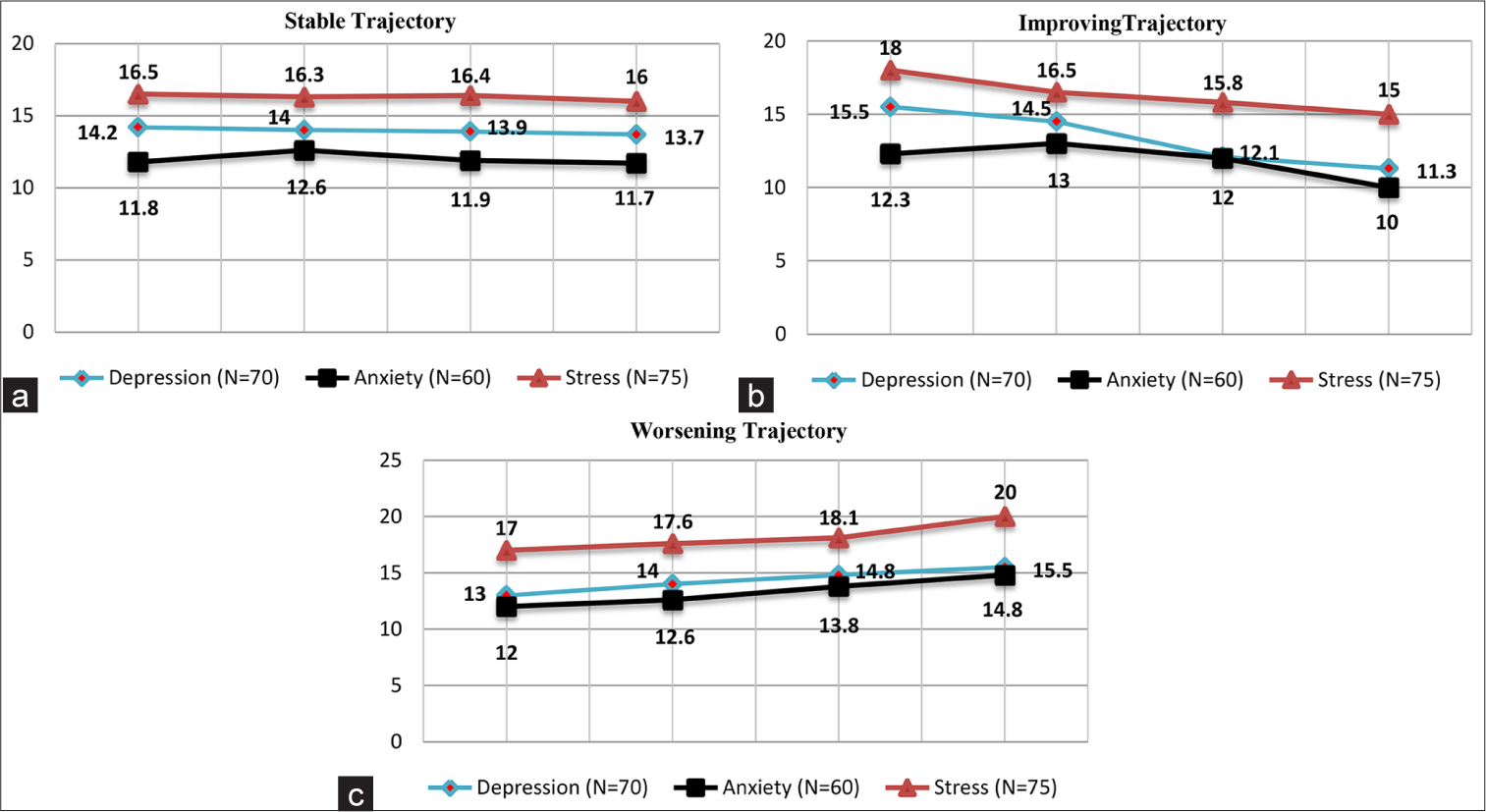
- (a) Stable trajectory of depression, anxiety, and stress, (b) improving trajectory of depression, anxiety, and stress, and (c) worsening trajectory of depression, anxiety, and stress. (a-c) X-axis: Time points (Baseline, 3 months, 6 months, 12 months). Y-axis: Symptom severity scores (Depression, Anxiety, Stress).
Improving Trajectory: Participants whose scores demonstrated a consistent decline by more than 1 SD across subsequent assessments. The improving trajectory group (n = 100, 50%) had initially high levels of depression at baseline (T1), but their scores gradually decreased over time. This indicates that these participants experienced an improvement in their depression symptoms as they moved further away from the time of diagnosis [Figure 1b]. Worsening Trajectory: Participants whose scores increased by more than 1 SD from their baseline values over time. The worsening trajectory group (n = 30, 15%) started with lower levels of depression at baseline (T1), but their scores increased over time. This suggests that these individuals experienced a worsening of depression symptoms over the 1st year following diagnosis [Figure 1c].
Trajectories of anxiety
Stable Trajectory (n = 60, 30%): Participants in this group experienced stable anxiety levels over the 1st year, with their scores remaining relatively consistent from baseline (T1) to 12 months (T4) [Figure 1a].
Improving Trajectory (n = 110, 55%): Participants in this group initially had higher anxiety scores at baseline (T1), but their scores gradually decreased over time, indicating an improvement in their anxiety symptoms [Figure 1b].
Worsening Trajectory (n = 30, 15%): Participants in this group began with lower anxiety scores at baseline (T1), but their scores increased as the year progressed, suggesting a worsening of their anxiety symptoms [Figure 1c].
Trajectories of stress
Stable Trajectory (n = 75, 37.5%): Participants in this group had stable stress levels over the 1st year, with their scores remaining relatively consistent from baseline (T1) to 12 months (T4) [Figure 1a].
Improving Trajectory (n = 100, 50%): Participants in this group initially had higher stress scores at baseline (T1), but their scores gradually decreased over time, indicating an improvement in their stress levels [Figure 1b].
Worsening Trajectory (n = 25, 12.5%): Participants in this group began with lower stress scores at baseline (T1), but their scores increased over the year, suggesting a worsening of their stress symptoms [Figure 1c].
Covariate analysis
Covariates, including age, socioeconomic status, cancer stage, and social support, were included in the growth curve models to assess their associations with the trajectories of depression, anxiety, and stress. The results indicated that age was significantly associated with the trajectories of depression (β = −0.28, P < 0.001), anxiety (β = −0.15, P < 0.05), and stress (β = −0.14, P < 0.05), suggesting that younger patients experienced greater improvements in psychological symptoms. Socioeconomic status also showed significant associations with depression (β = −0.12, P < 0.05) and anxiety trajectories (β = −0.10, P < 0.05), indicating that higher socioeconomic status was related to more favourable outcomes. Cancer stage and social support did not significantly impact the trajectories of these psychological symptoms (P > 0.05) [Table 3].
| Covariate | Depression (β) | Anxiety (β) |
Stress (β) |
|---|---|---|---|
| Age | −0.28* | −0.15* | −0.14* |
| Socioeconomic status | −0.12* | −0.10* | −0.05 |
| Treatment modality | 0.04 | −0.02 | 0.01 |
| Social support | −0.01* | 0.03 | 0.02 |
Interaction effect between time and age group
An important finding of this study was the significant interaction effect between time and age group on depression trajectories (P < 0.05). This interaction effect suggests that age moderates the rate of change in depression scores over time. Specifically, younger patients (ages 30–49) demonstrated a steeper reduction in depression scores from baseline (T1) to 12 months (T4) compared to middle-aged patients (ages 50–59) and older patients (ages 60+). However, no significant interaction effects were observed between time and age group for anxiety or stress trajectories (P > 0.05), indicating that the rate of change in anxiety and stress scores did not significantly differ across age groups. On the other hand, significant interaction effects between time and cancer stage (P = 0.023) on anxiety trajectories were observed. Patients with advanced cancer stages (Stages III and IV) showed a steeper decline in anxiety levels over time compared to patients with early-stage breast cancer. This indicates that patients with more advanced cancer experienced a more rapid improvement in anxiety symptoms as they progressed through the 1st year of diagnosis.
Post hoc analysis: Subgroup differences
Post hoc analyses using Bonferroni-corrected pairwise comparisons revealed that depression and Stress levels at the 12-month assessment were significantly lower compared to the 3-month assessment (P < 0.01) along with anxiety levels at the 12-month assessment (M = 8.7, SD = 3.2) were significantly lower than those at the 3-month (P < 0.001) and 6-month (P < 0.05) assessments [Table 4].
| Time points | Depression (P-value) | Anxiety (P-value) | Stress (P-value) |
|---|---|---|---|
| T1 versus T2 | 0.792 | 0.689 | 0.845 |
| T1 versus T3 | 0.309 | 0.177 | 0.419 |
| T1 versus T4 | 0.015* | 0.004* | 0.001* |
| T2 versus T3 | 0.871 | 0.714 | 0.861 |
| T2 versus T4 | 0.024** | 0.007* | 0.002** |
| T3 versus T4 | 0.038* | 0.012* | 0.003* |
Mixed effect modeling also revealed that the surgery-only group experienced a sharper decline in distress compared to the group receiving additional treatments. Besides this, individuals with high PSS demonstrated steeper declines in depression, anxiety, and stress levels compared to those with low PSS. The effect of PSS was significant for all emotional states (P < 0.05).
Overall, the results indicate that breast cancer patients experienced a significant reduction in depression, anxiety, and stress levels over the 1st year following diagnosis. However, individual differences in baseline levels and longitudinal trajectories suggest that targeted support may be beneficial for specific subgroups of patients. Further research is needed to explore additional factors influencing psychological outcomes in this population.
DISCUSSION
The present study aimed to investigate the trajectories of depression, anxiety, and stress among breast cancer patients during the 1st year following their diagnosis. The findings revealed significant changes in psychological outcomes over time, shedding light on the psychological challenges faced by breast cancer patients during this critical period and contributing to the growing body of literature addressing psychological well-being in cancer patients.
The identified trajectory groups – stable, improving, and worsening – align with previous research that has reported similar heterogeneous patterns of psychological symptoms among cancer patients.[3,13] Our study’s results underscore the need for individualised support strategies that account for the diverse trajectories, ensuring timely intervention for patients who may experience deteriorating psychological well-being. Interestingly, the observed interaction effect between time and age on depression trajectories echoes previous research in non-cancer populations, suggesting that younger individuals tend to show greater improvements in psychological symptoms over time.[5] However, our findings also highlight the importance of considering the specific context of cancer diagnosis, as younger patients may face unique challenges that impact their psychological responses differently than in non-cancer settings.
The post hoc analysis further reinforced the significance of trajectory groups in understanding psychological well-being dynamics. Our results align with studies indicating that individuals with stable trajectories tend to have better overall mental health outcomes,[14] emphasizing the potential benefit of early identification and intervention for patients at risk of worsening symptoms.
The observed heterogeneity in trajectories also suggests that not all breast cancer patients follow a uniform psychological recovery pattern. Consequently, healthcare professionals need to tailor psychosocial support interventions to address the specific needs of patients in different trajectory groups. Patients classified in the worsening trajectory may require more intensive and timely interventions to prevent further psychological deterioration. Conversely, patients in the stable or improving trajectory groups may benefit from supportive services that focus on maintaining their positive psychological outcomes or facilitating continued improvement.
In addition, the significance of socioeconomic factors has been highlighted. Low socioeconomic status, often linked to reduced access to resources and support, has been associated with heightened psychological distress.[15] The study results also emphasize the significance of providing early psychosocial support to breast cancer patients, particularly during the initial stages of diagnosis. The reduction in psychological distress over time suggests that early intervention and support may play a crucial role in promoting adaptive coping strategies and facilitating positive psychological outcomes. The pivotal role of age, as a potential moderator in psychological trajectories, is also evident in research by Esser et al. (2016),[5] emphasising that age-related differences might influence how patients cope with and respond to cancer-related stressors. Healthcare providers should be vigilant in identifying patients with higher baseline distress levels and provide timely interventions to prevent prolonged psychological suffering.
Thus, the reduction in psychological distress over time suggests that early intervention and support may play a crucial role in promoting adaptive coping strategies and facilitating positive psychological outcomes. Healthcare providers should be vigilant in identifying patients with higher baseline distress levels and provide timely interventions to prevent prolonged psychological suffering.
Therefore, this study advances our understanding of psychological trajectories among breast cancer patients and underscores the value of considering individual differences for tailored interventions. By recognising the diverse patterns of psychological responses and the moderating role of age, healthcare professionals can enhance the support offered to patients during a critical phase of their cancer journey, ultimately promoting better psychological well-being and overall quality of life.
Limitations and future directions
While this study provides valuable insights, several limitations warrant consideration. First, the assessment of psychological symptoms was limited to self-report measures, and potential confounding factors not explored in this analysis may contribute to trajectory variations. Future studies could incorporate objective measures and clinician assessments to provide a more comprehensive understanding of psychological well-being. Second, the study’s focus on the 1st year following diagnosis may not capture longer-term trajectories, underscoring the need for longitudinal studies encompassing extended timeframes. Third, the study focused on breast cancer patients in a specific geographic region, potentially limiting the generalizability of the findings. Future research could expand the study to include diverse populations to examine how cultural and social factors might influence psychological trajectories.
CONCLUSION
This study advances our understanding of psychological trajectories among breast cancer patients and underscores the value of considering individual differences for tailored interventions. By recognising the diverse patterns of psychological responses and the moderating role of age, healthcare professionals can enhance the support offered to patients during a critical phase of their cancer journey, ultimately promoting better psychological well-being and overall quality of life.
Acknowledgments
We would like to acknowledge the breast cancer patients who participated in this study. We are grateful for the support and cooperation received from the oncology clinics and hospitals. Special thanks to the medical and nursing staff for their assistance in patient recruitment and data collection. Finally, we express our heartfelt appreciation to our families, friends, and colleagues for their unwavering encouragement.
Ethical approval
The research/study was approved by the Institutional Review Board at the Institute of Medical Sciences, Banaras Hindu University, number ECR/Bhu/Inst/UP/2013/Reregistration2017dt.31.01.2017/No.Dean/2017/EC/24.10.2017, dated 24th October 2017.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- A longitudinal study of the effects of a hope intervention on levels of hope and psychological distress in a community-based sample of oncology patients. Eur J Oncol Nurs. 2011;15:351-7.
- [CrossRef] [PubMed] [Google Scholar]
- Proposing and evaluating a model of depression, stress, resilience and spirituality in relation to pain in women with breast cancer: Investigating the mediating role of mindfulness. Eur J Oncol Nurs. 2023;62:102268.
- [CrossRef] [PubMed] [Google Scholar]
- Anxiety, Depression and Quality of Life After Cancer Diagnosis: What Psychosocial Variables Best Predict how Patients Adjust? Psychooncology. 2012;21:857-67.
- [CrossRef] [PubMed] [Google Scholar]
- Trajectories of Anxiety and Depression Symptoms over Five Years since Breast Cancer Diagnosis: Results of the NEON-BC Prospective Study. Healthcare (Basel). 2022;10:661.
- [CrossRef] [PubMed] [Google Scholar]
- Risk and associated factors of depression and anxiety in men with prostate cancer: Results from a German multicenter study. Psychooncology. 2020;29:1604-12.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of age and emotional acceptance on distress among breast cancer patients. Support Care Cancer. 2007;15:73-9.
- [CrossRef] [PubMed] [Google Scholar]
- Manual for the Depression Anxiety Stress Scales (DASS) In: New South Wales. Australia: Psychology Foundation Monograph; 1995.
- [CrossRef] [Google Scholar]
- Depression Anxiety and Stress Scale: Reliability and Validity of Hindi Adaptation. Int J Educ Manag. 2013;3:446-9.
- [Google Scholar]
- Manual for PGI Social Support Questionnaire Varanasi: India Rupa Psychological Centre; 1998.
- [Google Scholar]
- Social Support and Treatment Outcome in Alcohol Dependence Syndrome in Armed Forces. J Clin Diagn Res. 2015;9:VC01-5.
- [CrossRef] [PubMed] [Google Scholar]
- Perceived Social Support and Re-admission: A Comparative Study in Re-admitted and Non-admitted Persons with Schizophrenia. Global Res Anal. 2013;2:194-6.
- [Google Scholar]
- Life Events, Social Support, Coping Strategies, and Quality of Life in Attempted Suicide: A Case Control Study. Indian J Psychiatry. 2013;55:46-51.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of Depression Severity with the PHQ-9 in Cancer Patients and in the General Population. BMC Psychiatry. 2016;16:22.
- [CrossRef] [PubMed] [Google Scholar]
- Subjective Well-being Mediates the Effects of Resilience and Mastery on Depression and Anxiety in a Large Community Sample of Young and Middle-aged Adults. Aust N Z J Psychiatry. 2011;45:240-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and associated factors of depression and anxiety among patients with cancer seeking treatment at the Butaro Cancer Center of Excellence in Rwanda. Front Public Health. 2023;11:972360.
- [CrossRef] [PubMed] [Google Scholar]




