
Translate this page into:
Sequential Supraclavicular Brachial Plexus and Stellate Ganglion Neurolysis for Upper Limb Pain in Metastatic Breast Cancer
Address for correspondence: Dr. Anil Kumar Paswan, Department of Anaesthesiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005, Uttar Pradesh, India. E-mail: dranil1973@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Neuropathic pain in cancer can result in severe debilitation to a patient with limited treatment options. Interventional modalities like nerve destruction can provide relief but at the expense of motor paralysis. Sympathetic pain is often an undiagnosed and undertreated condition that may accompany cases of chronic pain. We describe a case of severe neuropathic pain in brachial plexopathy in a middle-aged woman caused by metastatic breast cancer that was managed by chemical neurolysis of brachial plexus. Residual pain was treated by neurolysis of stellate ganglion due to the presence of sympathetic pain. This case report highlights the importance of the dual nature of pain and its management by chemical neurolysis in severe refractory neuropathic and sympathetic mediated pain.
Keywords
Brachial plexus
cancer pain
neurolysis
stellate ganglion
sympathetic mediated pain

INTRODUCTION
Cancer pain results in severe functional and psychosocial disability to a patient with increased economic burden. Opioids are the cornerstone of pain management in such patients with chemical neurolysis reserved for cases with severe intractable pain.[1] As many as 90% of the patients with advanced breast cancer need interventional pain management due to inadequate pain relief with pharmacological methods.[2] Pain caused by cancer can be visceral, neuropathic, somatic, or a combination of these. Sympathetic plexus neurolysis is commonly performed for various malignancies causing visceral pain, while that of somatic nerves is avoided as it results in side effects such as numbness and motor loss.[3] We describe a unique case where upper limb pain was managed by neurolysis of brachial plexus (somatic) and stellate ganglion (sympathetic) in metastatic breast cancer patient due to the dual nature of pain.
CASE REPORT
Our patient is a 45-year-old female diagnosed with left-sided breast cancer who underwent modified radical mastectomy with adjuvant chemotherapy and radiotherapy. One year later, she developed left supraclavicular lymphadenopathy, for which she received external beam radiotherapy. The patient was asymptomatic for 2 years after which she developed left arm pain and recurrence of supraclavicular lymphadenopathy. It was associated with lymphedema in the arm. The pain was initially dull aching, present in the shoulder region and arm. Over a period of 6 months, her pain increased and was accompanied by severe continuous, sharp, shooting pain and numbness for the past 1 month with a score of 9/10 on the Visual Analog Scale (VAS). She was taking oral medications for her pain which included tablet pregabalin 75 mg BD tablet aceclofenac/paracetamol 100/325 mg BD and tablet morphine which was gradually escalated to response at 240 mg/day over 6 months. She had developed constipation in response to morphine with severe refractory pain. Her supraclavicular lymph nodes were enlarged which were tender and indurated. She was unable to abduct the shoulder and flex the elbow with motor power of 2/5 in hand. Based on the clinical findings, the diagnosis of brachial plexopathy secondary to lymph node compression was made. Magnetic resonance imaging could not be done due to financial constraints. As the patient had very little motor power with no useful function of the arm, decision of diagnostic brachial plexus block, followed by neurolysis was made after taking informed consent from the patient. Under ultrasonographic guidance (USG) using a linear high-frequency probe (Sonosite M-Turbo™, Sonosite Inc., Bothell,_WA, USA), the supraclavicular block was performed using out-of-plane approach as the needle was unable to pass through the nodes due to induration along with distorted anatomy [Figure 1]. Block was performed with 22 G echogenic needle (50 mm Sonoplex– Pajunk™) and 10 ml of 0.25% bupivacaine was given. The patient had complete pain relief for 10 h. The next day, the patient was explained about the neurolytic procedure and the expected motor loss. Neurolysis was then performed with 12 ml of 75% ethanol and 0.125% bupivacaine resulting in 75% pain relief after 24 h with total motor loss of the arm. No phrenic nerve paralysis was seen. However, the patient still had pain in the arm which increased in the dependent posture. Assuming that the sympathetic pain component was responsible for the pain, we decided to go for diagnostic stellate ganglion block (SGB) under USG, injecting 6 ml 0.25% bupivacaine at C6 level below the prevertebral fascia and above the longus colli muscle using an in-plane technique. This resulted in complete pain relief for 6 h. Thereafter, informed consent was obtained from the patient, and stellate ganglion neurolysis was performed with 4 ml of 100% ethanol and 1 ml of 0.5% bupivacaine resulting in complete pain relief [Figure 2]. This resulted in warming of the ipsilateral hand and Horner's syndrome – ptosis, miosis, conjunctival congestion, and enophthalmos. The Horner's syndrome thus developed was permanent in nature, although the patient did not have any discomfort due to it. Low volume of 4 ml was chosen for this block to avoid unintentional spread to phrenic or recurrent laryngeal nerve. The patient was advised to use compression bandage for the management of lymphedema. The patient was followed at 1 and 2 months with sustained pain relief. Morphine was gradually tapered to 60 mg/day and the dosage of other medications was also reduced. Her VAS was 3/10 with the above medications and lymphedema was decreased marginally.
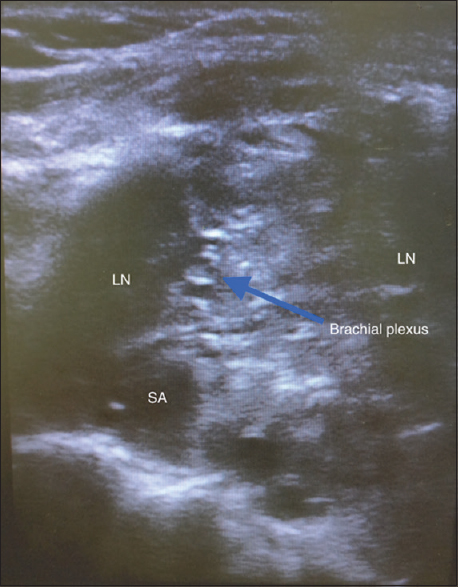
- Supraclavicular nerve block showing distorted anatomy. LN: Lymph node, SA: Subclavian artery
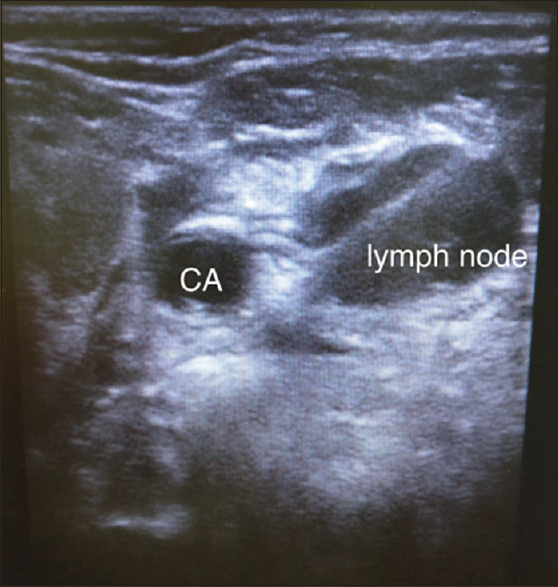
- Stellate ganglion block showing needle passing through the lymph node. CA: Carotid artery
DISCUSSION
Malignant brachial plexopathy is a debilitating condition caused commonly by metastatic breast, lung cancer, and radiation fibrosis. It results in severe neuropathic pain and motor loss of arm due to inflammation and compression/infiltration of nerves by tumor. Treatment is mainly conservative with chemotherapy and radiotherapy as options.[4] Oral medications such as gabapentin and pregabalin are used for neuropathic pain, whereas opioids are reserved for severe managing severe pain. In cases not managed by opioids or where they are not tolerated by the patient, interventional pain management takes predominance. For this, an accurate diagnosis should be made regarding the anatomic location and component of pain present.
For cancer pain involving the extremities, interventional pain management is limited to neuraxial (epidural and intrathecal) drug delivery systems. These, however, can be quite expensive, have many adverse effects, and need long-term close monitoring.[5] Somatic neurolysis is avoided as it results in sensory and motor loss and can lead to further patient disability. Brachial plexus neurolysis is not commonly described in the literature with few case reports citing its successful use. In a case of arm pain due to malignant peripheral nerve sheath tumor, neurolysis was performed with 20 ml 50% alcohol. The patient has 50% improvement in pain but decrease in opioid consumption was not seen.[6] Complete pain relief was achieved with infraclavicular brachial plexus neurolysis of lateral and posterior cord separately using 5 ml phenol (each block) in patient with soft-tissue sarcoma of the biceps muscle.[7] As these are somatic nerves, motor loss is invariably seen with the destruction of the nerves. In our case, we decided for the neurolysis as very little motor power was present. The procedure successfully resulted in >50% improvement in pain, especially the neuropathic component with lesser drug volume in blocks compared to the above cases.
In chronic pain conditions, sympathetic-mediated pain (SMP) may develop due to abnormal sprouting of sympathetic fibers on the somatic nerve fibers.[8] Diagnosing SMP is clinically challenging and it requires diagnostic sympathetic block. In our patient, residual dull continuous pain was present even after neurolysis which could suggest SMP component. This could have been because of the distorted anatomy of the brachial plexus preventing its complete destruction. As the plexus was not clearly visualized and anticipating SMP, we decided for diagnostic SGB which proved to be successful. Neurolysis of SGB poses some risks as inadvertent spread may result in recurrent laryngeal nerve paralysis. SGB has a role in breast cancer pain management as it has been used for lymphedema of the arm[9] and postmastectomy pain syndrome.[10] The mechanism by which it reduces lymphedema is supposedly the venous dilation leading to drainage of the excess fluid. Our patient reported slight decrease in lymphedema after the neurolysis of stellate ganglion. Arm and shoulder exercises, which are the mainstay of lymphedema management, could not be performed by the patient in view of motor loss before the intervention.
One challenge we faced was distorted superficial supraclavicular anatomy due to lymphadenopathy. We had to use out-of-plane approach as needle manipulation was not possible through the indurated lymph nodes. As there was a risk of phrenic nerve blockade and inadvertent spread, the total volume injected was kept to a minimum in both blocks to avoid complications.[1112] It is worthwhile to mention that radiofrequency ablation could have been performed for the brachial plexus block. We chose to proceed with the chemical neurolysis as the plexus was compressed and not visualized properly, and hence, it would have been difficult to locate all the trunks and incomplete lesion was a possibility. Brachial plexus neurolysis was performed before SGB as the patient had severe neuropathic pain component with motor loss.
This case report demonstrates effective brachial plexus neurolysis, followed by stellate ganglion neurolysis to treat SMP and is probably the first report where the combined block was used for treatment for upper limb pain. This report also highlights the importance of tailoring the approach for pain management as the neurolytic block was chosen as the first modality keeping in mind the absence of motor power in the arm. Achieving the desired pain management outcome includes the assessment of the character of pain and treating it accordingly.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The role of chemical neurolysis in cancer pain. Curr Pain Headache Rep. 2010;14:261-7.
- [Google Scholar]
- Prevalence of pain in patients with cancer: A systematic review of the past 40 years. Ann Oncol. 2007;18:1437-49.
- [Google Scholar]
- Evidence-based clinical practice guidelines for interventional pain management in cancer pain. Indian J Palliat Care. 2015;21:137-47.
- [Google Scholar]
- Intrathecal infusions for intractable cancer pain: A qualitative study of the impact on a case series of patients and caregivers. Pain Res Manag. 2009;14:371-9.
- [Google Scholar]
- Supraclavicular brachial plexus neurolysis for a malignant peripheral nerve sheath tumor: A case report. A A Pract. 2018;11:309-11.
- [Google Scholar]
- Selective infraclavicular brachial plexus phenol injection for the relief of cancer pain. Anesthesiology. 2015;122:1153.
- [Google Scholar]
- Progress in sympathetically mediated pathological pain. J Anesth Perioper Med. 2015;2:216-25.
- [Google Scholar]
- Effects of stellate ganglion block on breast cancer-related lymphedema: Comparison of various injectates. Pain Physician. 2015;18:93-9.
- [Google Scholar]
- Fluoroscopic stellate ganglion block for postmastectomy pain: A comparison of the classic anterior approach and the oblique approach. Clin J Pain. 2011;27:207-13.
- [Google Scholar]
- Effect of local anesthetic volume (20 mL vs.30 mL ropivacaine) on electromyography of the diaphragm and pulmonary function after ultrasound-guided supraclavicular brachial plexus block: A randomized controlled trial. Reg Anesth Pain Med. 2019;44:69-75.
- [Google Scholar]
- The optimal volume of 0.2% ropivacaine required for an ultrasound-guided stellate ganglion block. Korean J Anesthesiol. 2011;60:179-84.
- [Google Scholar]




