
Translate this page into:
Symptoms After Hospital Discharge Following Hematopoietic Stem Cell Transplantation
Address for correspondence: Dr. Semiha Akin; E-mail: semihaakin@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aims:
The purposes of this study were to assess the symptoms of hematopoietic stem cell transplant patients after hospital discharge, and to determine the needs of transplant patients for symptom management.
Materials and Methods:
The study adopted a descriptive design. The study sample comprised of 66 hematopoietic stem cell transplant patients. The study was conducted in Istanbul. Data were collected using Patient Information Form and Memorial Symptom Assessment Scale (MSAS).
Results:
The frequency of psychological symptoms in hematopoietic stem cell transplant patients after discharge period (PSYCH subscale score 2.11 (standard deviation (SD) = 0.69, range: 0.93-3.80)) was higher in hematopoietic stem cell transplant patients than frequency of physical symptoms (PHYS subscale score: 1.59 (SD = 0.49, range: 1.00-3.38)). Symptom distress caused by psychological and physical symptoms were at moderate level (mean = 1.91, SD = 0.60, range: 0.95-3.63) and most distressing symptoms were problems with sexual interest or activity, difficulty sleeping, and diarrhea. Patients who did not have an additional chronic disease obtained higher MSAS scores. University graduates obtained higher Global Distress Index (GDI) subscale and total MSAS scores with comparison to primary school graduates. Total MSAS, MSAS-PHYS subscale, and MSAS-PSYCH subscale scores were higher in patients with low level of income (P < 0.05). The patients (98.5%) reported to receive education about symptom management after hospital discharge.
Conclusions:
Hematopoietic stem cell transplant patients continue to experience many distressing physical or psychological symptoms after discharge and need to be supported and educated for the symptom management.
Keywords
Hematopoietic stem cell transplantation
Patient
Post-discharge
Symptoms

INTRODUCTION
Allogeneic and autologous hematopoietic stem cell transplantation (HSCT) is a lifesaving procedure which is frequently used not only for the treatment of hematological malignancies or diseases, but also as a therapy for solid tumors.[123] HSCT is type of treatment that includes the bone morrow, the peripheral blood, or the umbilical cord blood as a source of stem cells used for transplantation.[4] According to Turkish Transplant Registry, the approximate number of total transplants in 2005 and 2006 was reported to be above 800 per year. The numbers of HSCT patients and the transplant centers in Turkey are rapidly growing.[5]
HSCT produces increasing remission rates and improves survival.[6] HSCT improves the quality of life of patients with hematological malignancies.[47] Despite positive effects of this therapy, using chemoradiotherapy and immunotherapy for malignant and nonmalignant hematological disorders and HSCT procedure generate multiple problems and distress in all aspects of an individual's physical condition, emotional life, social life, and social interactions.[4891011] Long- and short-term effects of the HSCT can hamper the functional status and quality of life for HSCT patients.[8] After conditioning with high doses of chemoradiotherapy, patients following HSCT may face pancytopenia and infectious complications.[12] Allogeneic hematopoietic stem cell transplant survivors experience negative changes in their social life, sleep, and rest, and report tiredness, anxiety, sexual problems, changes of taste, dry mouth, sore mouth, appetite loss, and cough.[41314]
Patients and their families face significant physical and psychological stressors and changes during HSCT.[101516] Psychological distress is considered as a predictor of quality of life in cancer patients.[41718] Psychological distress and social problems can be sometimes more challenging for the patient, family, and healthcare team. Assessment of the psychosocial impact of transplant experience on patients and planning psychosocial interventions for meeting need is an integral for the management of psychosocial difficulties.[9] Identifying symptoms and factors that cause distress following HSCT, is important in early helping patients to improve their quality of life and their symptom management skills, and help patients to adjust to the consequences of HSCT, and enhance the response to the treatment.[1719] Communication, a multidisciplinary approach and long-term follow-up is important for the care of hematopoietic stem cell transplant patients.[2021]
MATERIALS AND METHODS
Study aims
The purposes of this study were to (1) assess the symptoms of hematopoietic stem cell transplant patients after hospital discharge, and (2) determine the care needs for symptom management of hematopoietic stem cell transplant patients.
The research questions were as follows:
-
What are the symptoms of transplant patients after hospital discharge following HSCT?
-
What are the variables associated with the symptoms observed in transplant patients after hospital discharge following HSCT?
Study design
This is a descriptive study. The research was conducted at the HSCT unit in a private hospital in Istanbul between November 2011 and January 2012.
Study sample
Population was made of 100 patients who had undergone hematopoietic stem cell transplant and were being followed-up after discharge. Patients were selected by convenience sampling. All patients who met the inclusion criteria were included into sample. Sample consisted of 66 patients who met the inclusion criteria and volunteered to attend the study. Inclusion criteria for sample were as follows: (1) Being at least 18-years-old, (2) undergoing HSCT, (3) being discharged following HSCT, and (4) giving consent to participate in the research.
Of 100 patients, 10 patients could be reached during visits to the clinic. Ninety patients were invited to participate into the study. Out of 90 patients, 19 were not willing to participate into the study and five patients had died. The study was conducted on remaining 66 patients. Five patients underwent allogeneic HSCT and 61 autologous HSCT.
Data collection
Institutional review board approval was obtained. The participants were given information about the study. They were invited to participate into study. Verbal informed consent was obtained from the patients. Researchers guaranteed anonymity.
Interview with the patient was conducted after the discharge period following HSCT. Interview was during patients’ hospital visit for routine follow-up. Data were collected using Patient Information Form and Memorial Symptom Assessment Scale (MSAS).
Data collection tools
Patient Information Form was prepared by the researchers. It contains questions about personal characteristics (e.g. age, gender, and marital status), health history (e.g. cigarette and/or alcohol use, history of chronic diseases, etc.), and disease- (type of cancer or disease, stage of cancer) and treatment-related characteristics (e.g. education about home-care after discharge, information about treatment, etc.). Patients were asked to rate their perception of health by giving points between 0 and 10 (0 = poor, 5 = moderate, 10 = very good).
Memorial Symptom Assessment Scale is a 32-item, patient-rated survey.[22] First 26 symptoms were rated in terms of frequency, intensity, and distress. The other six symptoms are rated in terms of intensity and distress. Memorial Symptom Assessment Scale comprises three subscales (MSAS-Global Distress Index (MSAS-GDI), MSAS-Physical Symptom Subscale Score (MSAS-PHYS), and MSAS-Psychological Symptom Subscale score (MSAS-PYSCH)). A 10-item MSAS-Global Distress Index (MSAS-GDI) measures the overall symptom distress. GDI is the average of the distress caused by four psychological symptoms (feeling sad, worrying, feeling irritable, and feeling nervous) and six physical symptoms (lack of appetite, lack of energy, pain, drowsiness, constipation, and dry mouth). MSAS-PHYS score is the average of the frequency, severity, and distress associated with 12 physical symptoms (lack of appetite, lack of energy, pain, drowsiness, constipation, dry mouth, nausea, vomiting, change in taste, weight loss, bloating, and dizziness). MSAS-PSYCH score is average of the frequency, severity, and distress associated with six psychological symptoms (worrying, feeling sad and nervous, difficulty in sleeping, feeling irritable, and having difficulty in concentrating). Total MSAS score is the average of symptom scores of all 32 symptoms on MSAS.[2223] Cronbach's alpha values of Turkish version of Total MSAS and MSAS subscales were between 0.71 and 0.84.[23] In this study, Cronbach's alpha value was 0.89 for total MSAS.
Data analysis
Data analyses were performed using Statistical Package for Social Sciences (SPSS) version 11.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics such as percentage, mean, standard deviation, and percentage were used for data analysis. One-sample Kolmogorov-Smirnov test was used to test the distribution of the data. Spearman's correlation analysis was used to compare symptoms scores with age. Mann-Whitney and Kruskal-Wallis tests were used to compare the mean values of scale scores with patients’ personal and disease-related characteristics. Tukey's post-hoc test was used to determine differences between group means.
RESULTS
Patients’ characteristics
More than half of the sample was (62.1%) male and married (84.8%). Mean age of study group was 46.38 (SD = 14.13, range: 18-71). Nearly half of the study group (47%) stopped working due to current disease or treatment.
The study group (97%) followed regularly their health check-ups as suggested by their physicians. The patients were asked to rate their perception of health condition for the last 1-year by giving points between 0 and 10 (0 = poor, 5 = moderate, 10 = very good). Patients described their health as poor (mean = 2.02, SD = 2.11, range 0-10). Nearly 20% of the group (18.2%) continued to smoke [Table 1].
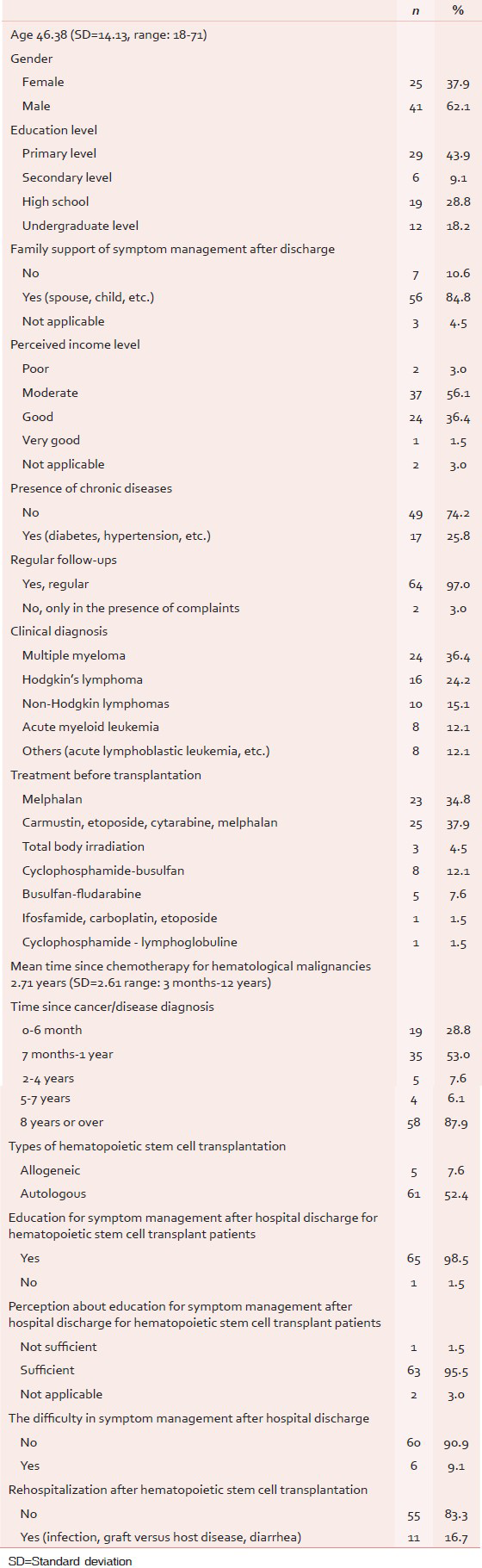
Patients’ disease and treatment-related characteristics
The patients had a history of multiple myeloma (36.4%), Hodgkin lymphoma (24.2%), non-Hodgkin lymphoma (15.2%), and acute myeloid leukemia (12.1%). Five patients underwent allogeneic HSCT and 61 autologous HSCT. Mean time since chemotherapy for hematological malignancies was 2.71 years (SD = 2.61 range: 3 months–12 years). The other clinical characteristics were presented in Table 1.
Almost all of the patients (98.5%) stated that the education for symptom management received after hospital discharge for symptom management was sufficient. Most of the patients (90.9%) stated that they did not experience some difficulties in coping with symptoms at home after hospital discharge [Table 1].
Symptoms after hematopoietic stem cell transplantation
Mean subscale scores of MSAS showed that the frequency of psychological symptoms (PSYCH subscale score 2.11 (SD = 0.69, range: 0.93-3.80)) were higher in hematopoietic stem cell transplant patients than frequency of physical symptoms (PHYS subscale score: 1.59 (SD = 0.49, range: 1.00-3.38)) [Table 2]. MSAS-GDI scores (mean = 1.91, SD = 0.60, range: 0.95-3.63) showed that overall symptom distress of caused by four psychological symptoms (feeling sad, worrying, feeling irritable, and feeling nervous) and six physical symptoms (lack of appetite, lack of energy, pain, drowsiness, constipation, and dry mouth) were at moderate level [Table 2].

A significant, positive and strong correlation was found between means of total MSAS and GDI subscale score (rs = 0.83, P < 0.01), and MSAS-PHYS subscale score (rs = 0.82, P < 0.01), and MSAS-PSYCH subscale score (rs = 0.80, P < 0.01). There were also positive and strong correlations among scores of each subscale scores [Table 2].
Most frequent six symptoms of current sample were difficulty sleeping, problems with sexual interest or activity, shortness of breath, feeling nervous, feeling drowsy, and worrying. The other frequent symptoms were diarrhea, lack of energy, feeling sad, cough, and itching. The most severe symptoms reported by patients were problems with sexual interest or activity, difficulty sleeping, shortness of breath, diarrhea, worrying, and feeling nervous. The most distressing symptoms were problems with sexual interest or activity, difficulty sleeping, diarrhea, hair loss, and problems with urination. These results show the patients who underwent stem cell transplantation with hematological malignancies need to be supported in management of various distressing physical or psychological symptoms [Figure 1 and Table 3].

- Frequency, severity, and distress of symptoms experienced by hematopoietic stem cell transplant patients

Variables associated with memorial symptom assessment scale scores
Statistically significant difference was found between total MSAS score, MSAS-GDI, MSAS-PHYS subscale, and MSAS-PSYCH subscale scores in terms of marital status (P > 0.05). Mean scores of total MSAS, MSAS-GDI, MSAS-PHYS subscale, and MSAS-PSYCH subscale were higher in single patients [Table 4].

Statistically significant difference was found between total MSAS score and MSAS-GDI subscale scores in terms of education level (P < 0.05). University graduates obtained higher GDI subscale and total MSAS scores with comparison to primary school graduates. However, no statistically significant difference was found between means of MSAS-PSYCH subscale and MSAS-PHYS subscale scores in terms of education level (P > 0.05) [Table 4].
Statistically significant difference was found between total MSAS scores and subscale scores in terms of personal perceived income level (P < 0.05). Total MSAS, MSAS-PHYS subscale, and MSAS-PSYCH subscale scores were higher in patients with low level of income [Table 4].
There was a statistically significant difference between total MSAS scores and subscale scores in terms of presence of an additional chronic disease (P < 0.05). Patients who did not have an additional chronic disease obtained higher scores [Table 4].
No statistically significant differences were found between MSAS scores in terms of gender, mean time since HSCT, and stage of cancer (P > 0.05). There were no correlation between scale scores and patients’ age (P > 0.05).
DISCUSSION
Patients diagnosed with hematological malignancies and who underwent hematopoietic HSCT has faced many long term problems during hospitalization and after and following hospital discharge. Patients with hematological malignancies commonly report lack of energy, hair loss, feeling sad, being oversensitive, numbness and tingling in hands and feet, change in taste, hair loss, pain, anorexia, feeling sleepy, anxiety, nausea, irritability, sleep disorder, perspiration, bloating, sexual disorders and loss of concentration.[24] Patients discharged following HSCT have to cope with various symptoms and problems caused by illness or treatment procedure.
Quality of life of patients underwent HSCT was affected by various symptoms and complications.[1314] Studies conducted on hematopoietic stem cell transplant patients reported that the patients experience physical symptoms, psychological problems, and changes in social life and relationships.[1125] A study conducted on Turkish patients underwent peripheral stem cell transplantation found that gastrointestinal problems (such as abnormal taste, nausea, vomiting, mouth sores, diarrhea, and constipation) and nervous system related symptoms (such as amnesia, loss of concentration, irritability and depression) were common.[26] Another study conducted on patients during the 1st year after allogeneic stem cell transplantation found that the most frequent symptoms were dry mouth, sore mouth, appetite loss, and change of taste.[413] Insomnia and sleep disruptions[2627] and anxiety, depression, changes in sexuality and tiredness[4142829] were among the other common complaints reported by stem cell transplant patients.
Current study results showed that the frequency of psychological symptoms were higher in hematopoietic stem cell transplant patients than frequency of physical symptoms. Overall symptom distress of caused by psychological symptoms and physical symptoms were at moderate level. Most frequent symptoms of current sample were difficulty sleeping, problems with sexual interest or activity, shortness of breath, feeling nervous, feeling drowsy and worrying, diarrhea, lack of energy, feeling sad, cough, and itching. Consistent with the other studies, the current study found that the most distressing symptoms were problems with sexual interest or activity, difficulty sleeping, diarrhea, and hair loss. These results show that patients underwent hematopoietic stem cell transplant patients due to hematological malignancies need to be supported in management of various distressing physical or psychological symptoms.
In a study conducted on patients with hematological malignancy, Mehrekula (2010) found a significant difference between total MSAS subscale scores in terms of gender.[24] Some other studies reported that women who had HSCT experienced various changes. Studies reported that female patients who underwent autologous stem cell transplantation experienced negative changes in their emotional status and sexual functioning.[1028] However, similar to study findings of Gürel (2007), the current found no statistically significant difference between total MSAS scores and subscale scores of stem cell transplant patients in terms of gender.[30]
Öz Sevli (2006) found statistically significant difference between emotional status scores in hematological malignancy patients in terms of marital status. Emotional dimension scores were higher scores in married patients than singles. On the other hand, single patients had higher scores from social life/family dimensions and activity level in comparison to the married patients.[31] In the current study, total MSAS scores were higher in single HSCT patients. This finding emphasizes the fact that single patients need more support about symptom management, and using social support sources efficiently is crucial especially for single patients.
Karacan (2006) reported that there was not statistically significant difference between anxiety and depression scores in terms of education level of peripheral stem cell transplantation patients.[26] The current study found that frequency of symptoms and symptom-associated distress were higher in patients with higher education level. In order to gain more knowledge about the relationship between education level and symptom distress, studies conducted on larger samples are needed.
A study conducted on patients with hematological malignancy found that as income level increased, the quality of life scores increased.[31] In the current study, total MSAS score, physical, and psychological subscale scores were found highest in patients with low level of income. This result indicates that the hematopoietic stem cell transplant patients with low-income level should be supported about symptom management.
Interestingly, this study found that the patients without additional chronic disease obtained higher scores from total MSAS and subscale scores. Patients with chronic diseases are likely to develop more effective strategies and self-confidence with management of symptoms due to illness or treatment. The study sample without another chronic disease might experience higher symptom frequency and symptom distress than patients with another additional chronic disease because patients without another chronic disease have less experience with coping with chronic disorders or treatment related problems.
Results show that the study sample who reported high incidence of symptoms described their health as poor. Those findings indicate the need of close and comprehensive symptoms and distress assessments and monitoring. Monitoring symptom distress during hospital stay and after discharge will help patient and health care team members to develop interventions and care plans for reducing patients’ symptoms distress and improve their quality of life at home and satisfaction with the treatment. Oncology nurses play a vital role in support patients, long-term survivors and their families.[20]
CONCLUSION
Frequency of psychological symptoms was higher in hematopoietic stem cell transplant patients than frequency of physical symptoms. Overall symptom distress of caused by psychological and physical symptoms were at moderate level. Most frequent symptoms of hematopoietic stem cell transplant patients after discharge were difficulty sleeping, problems with sexual interest or activity, shortness of breath, feeling nervous, feeling drowsy and worrying, diarrhea, lack of energy, and feeling sad.
Hematopoietic stem cell transplant patients in post-discharge period needed support and consultation for symptom management of distressing symptoms. Patient-family education and psychosocial support for symptom management for hematopoietic stem cell transplant patients after discharge should focus especially on management of fatigue, sleep disturbances and dyspnea. The current study showed that these patients need support and consultation services for managing with physical complaints and psychological symptoms and sexual disorders. Patient-specific planning is important for home-care period about assessment of symptoms, identification, and meeting care needs.
Study limitations
The most important limitation of the study is the size of the sample. The other limitation of the study is that the sample mainly comprises autologous hematopoietic stem cell transplant patients. So that the study results represent only the symptom distress of patients underwent autologous HSCT.
ACKNOWLEDGEMENTS
The authors are grateful to the patients for participating in the study.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Research priorities in haemato-oncology nursing: Results of a literature review and a Delphi study. Eur J Oncol Nurs. 2009;13:235-49.
- [Google Scholar]
- Hematopoietic stem cell transplantation in hematologic malignancies and solid tumours: Hacettepe University Institute of Oncology experience. Turk J Cancer. 2003;33:27-39.
- [Google Scholar]
- Quality of life in oncological and hematooncological patients after hematopoietic stem cell transplantation: The effect of selected psychosocial and health aspects on quality of life: A review of the literature. Rep Pract Oncol Radiother. 2007;12:53-9.
- [Google Scholar]
- Health-related quality of life, symptom distress and sense of coherence in adult survivors of allogeneic stem-cell transplantation. Eur J Cancer Care (Engl). 2001;10:124-30.
- [Google Scholar]
- Turkish Transplant Registry. Turkish transplant registry: A comparative analysis of national activity with the EBMT European Activity Survey. Bone Marrow Transplant. 2008;42(Suppl 1):S142-5.
- [Google Scholar]
- Is there still a role for allogeneic stem-cell transplantation in multiple myeloma? Best Pract Res Clin Haematol. 2007;20:783-95.
- [Google Scholar]
- Quality of life before and one year following stem cell transplantation using an individualized and a standardized instrument. Psychooncology. 2008;17:338-46.
- [Google Scholar]
- Symptoms and quality of life in diverse patients undergoing hematopoietic stem cell transplantation. J Pain Symptom Manage. 2012;44:168-80.
- [Google Scholar]
- Health-related quality of life in women with breast cancer undergoing autologous stem-cell transplantation. Cancer Nurs. 1996;19:368-75.
- [Google Scholar]
- Symptom distress, functional status and health-related quality of life before high-dose chemotherapy with stem-cell transplantation. Eur J Cancer Care (Engl). 2003;12:71-80.
- [Google Scholar]
- Home care during the pancytopenic phase after allogeneic hematopoietic stem cell transplantation is advantageous compared with hospital care. Blood. 2002;100:4317-24.
- [Google Scholar]
- Health-related quality of life in patients undergoing allogeneic stem cell transplantation after reduced intensity conditioning versus myeloablative conditioning. Cancer Nurs. 2009;32:325-34.
- [Google Scholar]
- Fatigue and physical activity in patients undergoing hematopoietic stem cell transplant. Oncol Nurs Forum. 2006;33:614-24.
- [Google Scholar]
- An individualized dyadic problem-solving education intervention for patients and family caregivers during allogeneic hematopoietic stem cell transplantation: A feasibility study. Cancer Nurs. 2010;33:E24-32.
- [Google Scholar]
- Distress in patients undergoing allogeneic haematopoietic stem cell transplantation is correlated with distress in nurses. Eur J Oncol Nurs. 2009;13:361-7.
- [Google Scholar]
- Predictors of health-related quality of life in patients treated with auto- and allo-SCT for hematological malignancies. Bone Marrow Transplant. 2012;47:757-69.
- [Google Scholar]
- Distress and quality of life after autologous stem cell transplantation: A randomized clinical trial to evaluate the outcome of a web-based stepped care intervention. BMC Cancer. 2010;10:361.
- [Google Scholar]
- Hematolojik Aciller ve Tedavileri (Hematological Emergencies and Management). XXX. Ulusal Hematoloji Kongresi, III. Hematoloji Ilk Basamak Kursu Kongre Kitabı. İstanbul: 30th National Hematology Congress, 3rd Hematology Course; 2003. p. :7-23.
- [Google Scholar]
- Survivorship issues in hematopoietic stem cell transplantation. Semin Oncol Nurs. 2009;25:159-69.
- [Google Scholar]
- Kemik iliği naklinin psikososyal boyutu (Psychosocial aspects of stem cells transplantation) Türkiye Klinikleri J Internal Med Sci. 2003;1:134-7.
- [Google Scholar]
- The memorial symptom assessment scale: An instrument for the evaluation of symptom prevalence, characteristics and distress. Eur J Cancer. 1994;30A:1326-36.
- [Google Scholar]
- Reliability and validity of the Turkish Version of the Memorial Symptom Assessment Scale in cancer patients. Asian Pac J Cancer Prev. 2011;12:3389-96.
- [Google Scholar]
- Hematolojik malignitelerde semptom kontrolü (Symptom management in hematological malignancies). Master's Dissertation, Ege Üniversitesi Sağlık Bilimleri Enstitüsü İç Hastalıkları Hemşireliği Anabilim Dali. In: İzmir;¸. Ege University Institute of Health Sciences Medical Nursing Department; 2010.
- [Google Scholar]
- Qualitative research on the patient's experiences following discharge after allogeneic hematopoietic stem cell transplantation aiming to develop a continuous patient support system. Rinsho Ketsueki. 2011;52:216-8.
- [Google Scholar]
- Periferik kök hücre nakli olan hastaların anksiyete ve depresyon düzeyi (Level of anxiety and depression in patients undergoing peripheral blood stem cell transplantation). Master's Dissertation, Hacettepe Üniversitesi Sağlık Bilimleri Enstitüsü ıç Hastalıkları Hemşireliği Programı. Ankara: Hacettepe University Institute of Health Sciences Medical Nursing Department; 2006.
- [Google Scholar]
- Sleep disturbance in hospitalized recipients of stem cell transplantation. Clin J Oncol Nurs. 2011;15:271-6.
- [Google Scholar]
- Sexuality following hematopoietic cell transplantation. Clin J Oncol Nurs. 2004;8:43-7.
- [Google Scholar]
- Impact of walking ability and physical condition on fatigue and anxiety in hematopoietic stem cell transplantation recipients immediately before hospital discharge. Eur J Oncol Nurs. 2012;16:26-33.
- [Google Scholar]
- Çukurova Üniversitesi Tıp Fakültesi Balcalı Hastanesi erişkin onkoloji, hematoloji kliniğinde kemoterapi uygulanan hastaların yaşam kalitesi ve bunu etkileyen faktörlerin incelenmesi (A Study on life quality and related factors of patients who take chemotherapy in the Units of Adult Oncology and Hematology of Cukurova University, Faculty of Medicine, Balcalı Hospital) Adana: Master's Dissertation, Çukurova University; 2007.
- [Google Scholar]
- Kemoterapi alan hematolojik malignansili hastalarda yaşam kalitesi (Quality of life and chemotherapy treated patients with hematological malignancy) Istanbul: Master's Dissertation, Marmara University; 2006.
- [Google Scholar]




