
Translate this page into:
The Effect of 5-Min Mindful Breathing on Pain in Palliative Care Cancer Patients: A Randomized Controlled Study
Address for correspondence: Dr. Ng Chong Guan, Department of Psychological Medicine, Faculty of Medicine, University Malaya, Lembah Pantai, 50603 Kuala Lumpur, Malaysia. E-mail: chong_guan@um.edu.my
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
While pain is a common complaint among palliative cancer patients, there is little research looking into nonpharmacological methods for the reduction of pain in the palliative setting.
Aim:
This study aims to study the efficacy of 5-min mindful breathing for rapid reduction of pain in a palliative care setting.
Methods:
This is a sub-analysis of the previous randomized controlled study on distress reduction. Sixty patients were recruited and randomly assigned to either the intervention (5-min mindful breathing) or the control (5-min normal listening) group. Participants reported their pain on a 10-item analog scale at baseline, immediately after intervention and 10 min postintervention. Changes in pain scores were further analyzed.
Results:
Pain scores decreased for both the intervention and control groups. However, the reduction of pain did not reach statistical difference in both groups (P > 0.05).
Conclusion:
Five-minute mindful breathing is a quick and easy to administer therapy but does not have significant effects in terms of pain reduction in palliative settings. Future research and directions are nonetheless suggested and encouraged to look for short-term mindfulness-based therapies on pain reduction for this population.
Keywords
Breathing
cancer
distress
mindfulness
pain

INTRODUCTION
Patients with terminal illnesses such as cancer frequently experience fluctuating levels of pain and psychological distress. These are further accompanied by feelings such as despair, depression, and hopelessness, which often makes the final stages of terminal illnesses a highly challenging and emotional time. The objective of palliative care is to improve the quality of life for patients and their families, with a focus on providing relief from symptoms, pain, and other stressors resulting from their illness. While palliative care can be appropriate at any age or stage in serious illnesses, it is crucial support for both the patient and their family members, particularly during end-of-life care.
In the management of cancer-related pain, nonpharmacological interventions such as psychotherapy or relaxation methods are of particular interest due to their lack of medical interactions and serious adverse events. Among them, recent years have seen increased attention on mindfulness-based interventions. Being mindful allows individuals to observe one's own feelings and thoughts from a distance, without attaching meaning to them; this allows thoughts and emotions to occur naturally without any attempt to suppress or switch them off.[1] Consequently, individuals can gain better awareness and thus respond to a situation with conscious choice rather than usual automatic, often negative reactions. This then promotes a less negative re-evaluation of an unpleasant situation and better emotion regulation.[1234]
With regard to pain management, mindfulness does not entail diversion but rather encourages us to stay with painful experience while being less reactive. In mindful breathing, one of the central and anchoring practices in mindfulness, participants are guided to rest their attention on their breathing. By experiencing each breath as they inhale, exhale, and repeat, breathing serves as an anchor that brings the them back to the present moment and helps them enter a state of awareness about their own negative thoughts and emotions. This increased state of awareness then allows them to respond mindfully, shifting their focus from pain back to the present moment.[1] Individuals are then able to respond consciously and nonjudgmentally to pain in the observation of their unpleasant thoughts; helping them realize that the pain may not be the sole reality but may be shaped by their thoughts as well.[567] In this sense, mindfulness helps not in reducing sensory pain but rather by providing a way for individuals to better control the cognitive and emotional aspects of pain, by minimizing the response to unpleasant mental experiences and by redirecting thoughts of burdening pain sensations to nonharmful sensory signals.[8] Being mindful and focusing on the “right-here-right-now” can hence break the cycle of rumination and worry, reducing the level of distress associated with pain and the stimulus as a result.[1]
Previous research in this area has yielded promising results as well. For instance, a study by Garland et al.[8] found that individuals showed relatively lower levels of pain severity and increased perceived control over their pain after carrying out mindfulness training. These results persisted up to 3 months following treatment and were tied to key therapeutic mechanisms such as mindful disengagement from negative appraisals and reduced affective bias in the reorientation of attention onto interoceptive information.[8] In addition, an experiment conducted by Zeidan et al.[2] which utilized electrical stimulation as experimentally induced pain, indicated that a brief 3-day mindfulness meditation training was effective in reducing pain sensitivity, subjective pain ratings to both high and low pain stimuli, as well as in reducing anxiety scores compared with baseline, relaxation, and distractions. A systematic review on mindfulness-based interventions for chronic pain in 2011 based on ten studies also concluded that mindfulness-based interventions could be useful for reducing depressive symptoms and improving specific psychological distress associated with chronic pain without modifying the pain itself.[3]
Most mindfulness-based interventions, however, can be challenging to employ and this is especially true in palliative care settings where patients and their families often experience fluctuating states of mental distress, physical impairment, and financial stress. Mindfulness-based stress reduction (MBSR) programs, for example, usually span 8 weeks and require trained professionals as well as daily homework.[9] Nonetheless, the past research has shown the potential for mindfulness-based interventions in increasing the quality of life of palliative care patients through a number of psychological factors, such as psychological distress,[7] perceived disability and pain[91011] affective response to pain stimuli.[12] In addition, a systematic review and meta-analysis conducted on 30 randomized controlled trials by Hilton et al.[13] surmised that type of intervention, medical condition, and length or frequency of intervention did not affect the efficacy of mindfulness meditation on pain, suggesting that shorter interventions may be equally as beneficial as MBSR in this respect. With these in mind, this intervention is structured to be 5 min long with a focus on mindful breathing, a core mindfulness practice. A previous research examining the efficacy of this 5-min mindful breathing intervention on distress reduction in palliative care patients found promising results, with this short intervention significantly reducing their distress after a single session.[714] As psychological distress has been found to correlate with the experience of pain, further investigation of this 5-min mindful breathing intervention in terms of pain reduction is warranted. Thus, the aim of the current study is to examine the efficacy of 5-min mindful breathing for pain reduction in palliative cancer patients.
The present study hypothesizes that there will be a significant reduction of pain in the 5-min mindful breathing group as compared to the control group.
METHODS
This is a subanalysis of a larger parallel-group, nonblinded, and randomized controlled study conducted in the palliative care unit of a public university hospital in Malaysia. The previous study examined the efficacy of 5-min mindful breathing technique in terms of distress reduction within that population.[14] Ethical approval was obtained from the University of Malaya Medical Centre Medical Research Ethics Committee prior to study commencement. There were no harms or unintended side effects from either the intervention or control in this study. Written consents were obtained from all participants and all information was kept confidential.
The inclusion criteria for this study were: (1) aged 18 years and above, (2) diagnosed with cancer of any type, (3) currently receiving palliative care, (4) reported a distress score of more than 4 on the distress thermometer, (5) able to understand and follow simple instructions, and (6) consented. The exclusion criteria were: (1) those who were delirious or confused, (2) those with breathing difficulties/respiratory distress and (3) those unable to maintain concentration for at least 20 min (based on subjective assessment by researcher during the process of interview and explanation of the study).
Patients from the palliative care unit were approached and screened for eligibility. Sixty of those fulfilled the above criteria and were recruited into the study. The nature of the study was then explained to their family members and care-takers. Their sociodemographic background information was collected while relevant clinical data (type of cancer, other comorbid medical conditions, and medications) were obtained from medical records. The sample size of this study is equivalent to that of the larger study, which was calculated based on the effect sizes of its earlier pilot study.7
The current study focused solely on changes in pain severity. This was measured using a 10-point analogue scale, in which 0 indicated “no pain at all” while 10 indicated “severe pain.” Higher scores indicated higher level of pain.
Procedure
Once consented, a baseline measurement of pain was taken using the 10-point analog scale at the beginning of the session (T1). Subjects were then randomly assigned to either the intervention arm (5-min mindful breathing) or the control arm (5-min normal listening) based on computer-generated random numbers with a 1:1 allocation ratio. Participants allocated to the intervention arm were guided through a 5-min mindful breathing technique while those allocated to the control arm were interviewed using a list of semi-structured questions for 5 min. The instructions and questions are presented in more detail in Appendix 1. Both sessions were guided by the researchers who were psychiatrists trained in mindfulness therapy. On completion, pain was reassessed immediately after the session (T2) and once again after a short break of 5–10 min (T3).
Statistical analysis
The primary analysis was done for the within-group changes in pain score from T1 to T2 and T1 to T3 for each group using Student's t-test. The secondary analysis compared the between-group (intervention vs. control) change in pain score for both T1 to T2 and T1 to T3 using Mann–Whitney. The objective was to see which group had the more significant and hence effective pain reduction. All tests were two tailed with a significance level of 0.05. Analyses were performed using SPSS Statistics for Windows, version 12.0 (SPSS Inc., Chicago, Ill., USA).
RESULTS
All 60 patients recruited completed their participation in the study. Figure 1 shows an overview of the flow from subject recruitment to completion of the study. Participants were mostly Chinese, married, middle-aged and were diagnosed with varying types of cancer [Table 1]. Pain score decreased at T2 and T3 compared to T1 for both the intervention and control groups. For the intervention group, there was further reduction from T2 (M = 3.65) to T3 (M = 3.48) while for the control group, there was no further reduction from T2 (M = 3.93) to T3 (M = 3.93). However, the results showed that the reduction of pain sensation through both 5-min mindful breathing and normal listening did not reach statistical significance [Table 2]. No adverse events occurred during or as a result of the study.
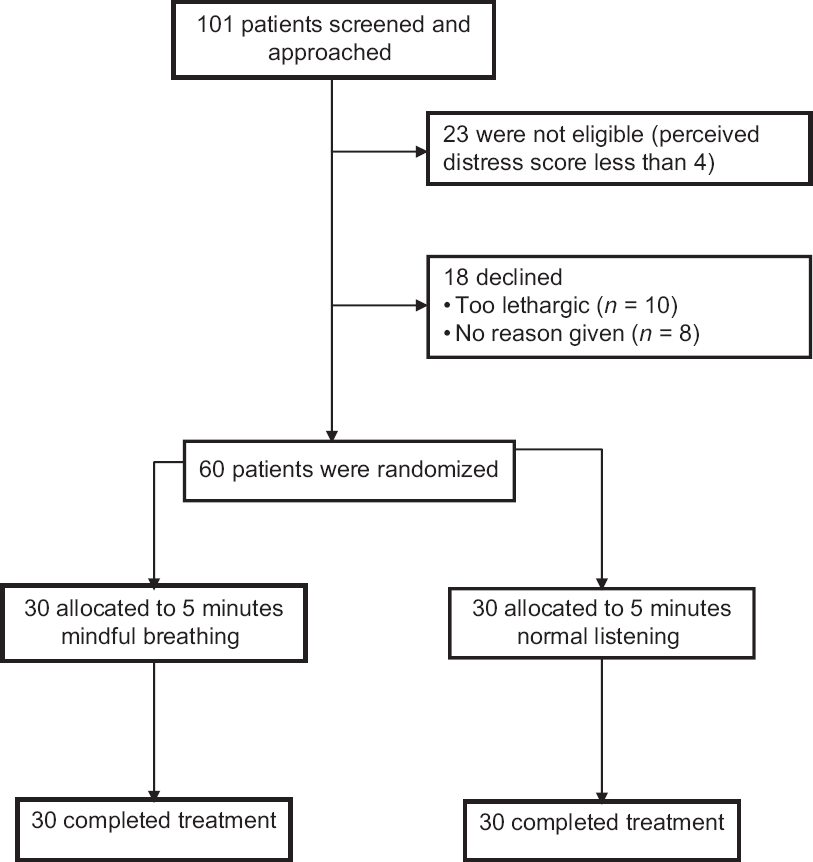
- Disposition of patients in the randomized controlled trial between 5 min mindful breathing and normal listening for cancer patients under palliative care
| Characteristics | |
| Age (years), mean (SD) | 47.03 (16.46) |
| Gender, n (%) | |
| Male | 29 (48.30) |
| Female | 31 (51.70) |
| Ethnicity, n (%) | |
| Malay | 14 (23.3) |
| Chinese | 36 (60.0) |
| Indian | 9 (15.0) |
| Others | 1 (1.7) |
| Religion, n (%) | |
| Muslim | 14 (23.3) |
| Buddhist | 24 (40.0) |
| Christian | 12 (20.0) |
| Hindu | 8 (13.3) |
| Others | 2 (3.3) |
| Marital status, n (%) | |
| Single | 19 (31.7) |
| Married | 41 (68.3) |
| Type of cancer, n (%) | |
| Breast | 10 (16.7) |
| Bone | 11 (18.3) |
| Lungs | 6 (10.0) |
| Hepatopancreatic | 4 (6.6) |
| Esophageal | 2 (3.3) |
| Nasopharyngeal | 6 (10.0) |
| Prostate | 3 (5.0) |
| Testicular | 3 (5.0) |
| Brain | 2 (3.3) |
| Cervical | 1 (1.7) |
| Others | 12 (20.0) |
SD: Standard deviation
| Intervention arm: 5 min mindful breathing | Five minute mindful breathing versus normal listening | ||||||
|---|---|---|---|---|---|---|---|
| 1, mean (SD) | 2, mean (SD) | 3, mean (SD) | 1- T2 (P) | 1- T3 (P) | (T1- T2) versus (T1’- T2’) (P) | (T1- T3) versus (T1’- T3’) (P) | |
| Pain | 4.12 (2.62) | 3.65 (2.50) | 3.48 (2.49) | 0.46 | 0.32 | N/A | N/A |
| Control arm: Normal listening | |||||||
| T1’, mean (SD) | T2’, mean (SD) | 3’, mean (SD) | T1’- T2’ (P) | T1’- T3’ (P) | |||
| Pain | 4.17 (2.62) | 3.93 (2.37) | 3.93 (2.37) | 0.72 | 0.72 | ||
T1: Beginning of the session, T2: Immediately after completion of the session, T3: 5- 10 min after completion of session, SD: Standard deviation, N/A: Between group analysis were not done as reduction of pain within group was not statistically significant
DISCUSSION
The results of the current study showed that both the 5-min mindful breathing (intervention) and 5-min normal listening (control) did not significantly reduce pain among the subjects. Our hypothesis suggesting that there will be a significant reduction of pain in the 5-min mindful breathing group compared to the control group was not supported.
There are some limitations to our study that may explain our findings. First of all, the present study is a subanalysis based on the previous randomized controlled trial, which found a that the 5-min mindful breathing intervention significantly reduced psychological distress in patients.[14] We hypothesized that along with distress reduction, the same mindful breathing technique would aid in the reduction of the subjective perception of pain. This is based on the contemporary notion that pain perception is linked to various psychological factors and thus, pain reduction would function similarly to or rely on similar mechanisms as in distress reduction. For instance, one's beliefs and attitudes, as well as focus and interpretation of noxious stimuli has been found to affect how pain is experienced and continues to develop.[10]
Nonetheless, while it is common for distress and pain to occur concurrently as well as correlate highly, it may be too simplistic to equate psychological distress to pain perception. For instance, the relationship between distress and pain perception has been found to involve multiple cognitive factors, such as catastrophic thinking and a sense of self-efficacy.[11] As such, the relationship between them, while a correlation, may be more complex than it originally appears. Second, another potentially influencing factor is our oversight in excluding trait positive and negative affect as part of our scope of research. Individuals with trait positive affect have been found to experience greater reduction of pain compared to those with trait negative affect.[12] It is possible that there may have been an imbalance in these traits within the randomly assigned groups, further contributing to the results.
In addition, the short intervention and observation period in our study, while necessary due to the challenges faced by our study population, may have contributed to the nonsignificant results. While both are influenced by psychological variables, pain perception is likely to have a stronger biological origin compared to psychological distress, which largely depends on how people interpret an unpleasant stimulus. The 5-min mindful breathing intervention as well as 5–10 min observation period thus may have been too short a duration to induce and sensitively pick up reduction in pain compared to the case with distress. A longer duration may have been needed for both the intervention and observation in order to accurately show efficacy.
It should also be noted that pain ratings were generally on the lower end of severity for both groups. Thus, possibly explaining the lack of significance in pain reduction compared to the baseline. Though not at a statistically significant level, participants did report some reduction in pain perception immediately after the 5-min mindful breathing intervention. The pain was further reduced shortly after the completion of the breathing exercise (5–10 min later). In addition, pain reduction, while not significant, was greater in the intervention group compared to the control group, suggesting that the intervention may pose some merits over the control at least. Lowered breathing rate is an integral part of mindfulness-based interventions, particularly in terms of mindful meditation, which is known to decrease anticipatory anxiety and pain perception.[15] This meditative state, however, often occurs together with a sense of relaxation. As our control condition involved normal listening based on semi-structured questions, it is possible that a relaxed state may have been induced in this condition, thus possibly accounting for the current results. We are further unable to determine if the results were due to mere relaxation or mindfulness as we did not include measures to check for these, in order to reduce possible fatigue effects in an already vulnerable population.
Furthermore, our sample size was rather small at only 60 participants as it was calculated based on a previous study that focused on the efficacy of 5-min mindful breathing on perceived distress rather than pain. As pain is relatively unexplored compared to psychological distress within this context, a larger sample size along with a longer duration of study is needed to properly examine the proposed aims and hypotheses, while also increasing the generalizability of the potential findings.
Perhaps another limitation of our study, was our decision to focus on pain severity for our pain outcome, as does the majority of past research. This, however, has been criticized recently in terms of its indirect effects in relation to mindfulness-based therapies, as well as its lack of clinical significance.[1617] Recent studies have argued that pain interference, the degree to which pain sensations interfere with daily life, may be a better indicator of the aim of acceptance- and mindfulness-based therapies compared to pain severity.[16] With relation to mindfulness-based therapy, patients are taught skills to increase their acceptance toward pain sensations rather than fight them, thus relating to a decrease in pain interference rather than pain severity.
Nigol and di Benedetto[17] found similar results with regard to pain severity and pain interference as treatment outcomes in examining the facets of mindfulness. They further found that differing facets of mindfulness had differing effects on pain: observing and describing directly affected pain, while nonjudgment, nonreactivity and describing indirectly affected pain through depression. A study conducted by Wood et al.[18] within a population of breast cancer patients found an association between the current metastatic site and pain severity as well as interference, with higher pain severity and greater pain interference reported by patients with both visceral and bone metastases compared to each metastasis individually. Wood et al.[18] further included a measure of health utility as well as general health status (mobility, self-care, and anxiety/depression), finding a negative correlation between these variables with both pain severity and interference, indicating a link between health status and pain outcomes. The findings additionally indicated that increased levels of anxiety and depression were associated with chemotherapy, which suggests that stage of cancer as well as stage of treatment could influence the perception of pain as well. Without accounting for these in the present study, it is difficult to accurately examine whether mindfulness-based interventions may indeed be effective in helping with pain in this setting. These suggests a need for future research in examining both different outcome measures of pain, performance and health status measures, as well as the efficacy of different facets of mindfulness on those outcomes.
CONCLUSION
While the present study did not manage to find a significant effect of the 5-min mindful breathing intervention on pain reduction, it does not negate its potential efficacy in light of past research. Shorter nonpharmacological treatment alternatives may greatly benefit patients in palliative care settings due to challenges they face in terms of cost, time, as well as their disadvantaged physical, mental and emotional capacity. In addition, while not significant, pain reduction was greater for those who practiced the 5-min mindful breathing intervention compared to those in the 5-min listening condition. This suggests the need for further research addressing the above and in examining different outcome measures of pain as well as the efficacy of different facets of mindfulness.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to thank all the patients and their family members who participated in the study.
REFERENCES
- The effects of brief mindfulness meditation training on experimentally induced pain. J Pain. 2010;11:199-209.
- [Google Scholar]
- Mindfulness-based interventions for chronic pain: A systematic review of the evidence. J Altern Complement Med. 2011;17:83-93.
- [Google Scholar]
- Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychol Inq. 2007;18:211-37.
- [Google Scholar]
- What are the benefits of mindfulness. A practice review of psychotherapy-related research? Psychotherapy. 2011;48:198-08.
- [Google Scholar]
- Mindfulness-based stress reduction for low back pain. A systematic review. BMC Complement Altern Med. 2012;12:162.
- [Google Scholar]
- Distress reduction for palliative care patients and families with five-minute mindful breathing: A pilot study. Am J Hosp Palliat Care. 2016;33:555-60.
- [Google Scholar]
- Mindfulness-oriented recovery enhancement for chronic pain and prescription opioid misuse: Results from an early-stage randomized controlled trial. J Consult Clin Psychol. 2014;82:448-59.
- [Google Scholar]
- Differential engagement of anterior cingulate and adjacent medial frontal cortex in adept meditators and non-meditators. Neurosci Lett. 2007;421:16-21.
- [Google Scholar]
- Impact of psychological factors in the experience of pain. Phys Ther. 2011;91:700-11.
- [Google Scholar]
- Psychological distress is associated with greater perceived disability and pain in patients presenting to a shoulder clinic. J Bone Joint Surg Am. 2015;97:1999-2003.
- [Google Scholar]
- The effects of slow breathing on affective responses to pain stimuli: An experimental study. Pain. 2010;149:12-8.
- [Google Scholar]
- Mindfulness meditation for chronic pain: Systematic review and meta-analysis. Ann Behav Med. 2017;51:199-213.
- [Google Scholar]
- The effect of 5 minutes of mindful breathing to the perception of distress and physiological responses in palliative care cancer patients: A randomized controlled study. J Palliat Care. 2016;19:917-24.
- [Google Scholar]
- Pain attenuation through mindfulness is associated with decreased cognitive control; and increased sensory processing in the brain. Cereb Cortex. 2012;22:2692-702.
- [Google Scholar]
- Acceptance And mindfulness-based interventions for the treatment of chronis pain: A meta-analytic review. Cogn Behav Ther. 2016;45:5-31.
- [Google Scholar]
- The relationship between mindfulness facets, depression, pain severity and pain interference. Psychol Health Med. 2020;25:53-63.
- [Google Scholar]
- Patient-reported pain severity, pain interference and health status in HR+/HER2- advanced/metastatic breast cancer. ESMO Open. 2017;2:e000227.
- [Google Scholar]




