
Translate this page into:
How “Elderly Staying Alone” Cope Up with their Age and Deteriorating Health: A Qualitative Exploration from Rural Wardha, Central India
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
This study is done to explore the various changes and problems faced by the “elderly people staying alone” and how they cope up to maintain their life amidst the physical, familial, social, and financial crisis in their lives.
Materials and Methods:
This qualitative study was carried out in the villages surrounding Bhidi Rural Health and Training Center, located in the Vidarbha region of Maharashtra. A triangulation of free listing and pile sorting exercise was used. Elderly >65 years of age of either sex, living alone in their own houses, for at least 2 years were included in the study. Twenty-four such individuals were selected purposively who could figure out the different words and concepts regarding the three domains of our study for the purpose of line listing, namely, change of life since staying alone, problems faced while staying alone, and how they cope up with the problem of living alone. The data were analyzed using Anthropac software. The study findings were presented to the participants, who later pointed out few recommendations to be made.
Results:
The “elderly staying alone” face the problems of lack of family, social, and financial support in their day-to-day life. They cope with these problems by a number of ways. Although there are a number of government schemes to protect the elderly, none of these policies are dedicated to this special group of elderlies.
Conclusion:
There is no social structure that can take care of this vulnerable group of elderlies in rural India. It is high time for the government to step in to bring some societal and familial reforms that will safeguard the elderly staying alone from the ongoing familial, social, and financial hardship.
Keywords
Cope up
elderly staying alone
problems faced
rural India

INTRODUCTION
Aging is a physiological phenomenon. Due to the shift of the disease pattern from communicable to noncommunicable disease, easy availability of better health-care facilities, and increased disease prevention activities, the longevity of human beings has increased throughout the globe including India.[12] The United Nations Department of Economic and Social Affairs[3] projected that the elderly population in India is going to rise from 8% in 2015 to 11.5% in 2025 and 19% in 2050. They have also projected the old-age dependency ratio for India to increase from 9/100 (2015) to 11/100 (2025). Now, as the population is increasing, the demand for earning livelihood is increasing and becoming more tough making younger generation leave their homes and settle in distant urban localities to earn and send money to their elderly parents. As a result of which, unlike older times, elderly people are gradually becoming lonely and staying in solitude in their houses.[4] As people get older, they get vulnerable to different medical and psychological problems.[5] The World Health Organization[6] estimated that the overall prevalence rate of depressive disorders among the elderly generally varies between 10% and 20% depending on the cultural scenarios, the condition deteriorates when they lose their partners and are left completely alone in the family. According to the last census,[7] around 15 million elderly live all alone and three-fourth of them are women.
Conventionally, in India, the elderly have always been treated with great respect and occupied a prominent position in the family. While the younger generation felt duty bound to serve them, In rural India, joint family system is still prevalent, but in search of jobs, there are increasing migrations of younger generation from rural to urban localities leaving the elderly in their homes all alone.[8] The problem increases when there is nobody to take care of them in the villages. Rural India still lacks a facility to hire a caregiver or a nurse, who would take care of the elderly people living alone. There are not enough old age homes,[9] especially in Indian villages, where the old man or woman could spend his or her last days of life in peace, with someone to take care of them. Hence, it is the left alone elderly population, who has to do the daily chores of life and also take care of own selves till they die. There is a lack of studies about how “elderly people staying alone” cope with their deteriorating health in rural India. This qualitative study was hence planned to acquire a more comprehensive understanding of how the life of elderly people has changed since they were living alone; the problems they face and how did they cope up with those problems.
MATERIALS AND METHODS
Study settings
The present formative research was carried out in the surrounding villages of the rural health training center Bhidi, which is located in Wardha district of Vidharba region, about 750 km from the state capital, Mumbai. The elderly population who stayed alone in the villages are gradually increasing in number.
Study population
The selection of the respondents was based on the following criteria:
-
Elderly >65 years of age of either sex, living alone in their homes, for at least 2 years
-
Elderly people who were able to complete a normal conversation and tell about their experiences.
Sampling technique
Twenty-four elderly individuals of >65 years of age were selected purposively who could figure out the different words and concepts regarding the three domains of our study for the purpose of line listing, namely:
-
Change of life since staying alone
-
Problems faced while remaining alone
-
How did they cope up with the problem of living alone?
Elderly individuals of both sexes who voluntarily consented by themselves were included for the interview.
Procedure
We used two data collection methods for our study. Those were free listing and pile sorting, which was conducted by the author, trained in qualitative methods. Free listing was conducted in a language the study participants understood. Help of social worker was taken to identify such elderly individuals who stayed alone. All the interviews were conducted in the houses of the individuals maintaining adequate privacy.
The moderator explained the procedure of line listing and pile sorting and also the objective of our study to the participants individually before beginning the procedure.
Free listing is the technique of collecting relevant data in the form of words or small statement pertaining to the study objectives. The study participants were interviewed in accordance with our study objectives and their responses were free listed one by one.
Following free listing, we found out the key words or the statements that formed the units of pile sorting, specific to each of the three domains. Those units (composed of key words or small sentence) were written down in separate cards of three distinct colors. Participants were asked to sort out the unstructured pile of cards in response to each of the three domains and group these unsorted cards into one or more piles using any common characteristic. The reason for sorting the piles under one heading was explained by the participants and separate heading or title was given to each of the sorted piles. They were also asked to find out or sort any recommendations for the problems identified in pile sorting. Pile sorting helped in identifying items (or themes) that existed within our study objective. To do the pile sorting, we have again purposively selected individuals who could sort the cards into specific piles with proper reasoning. Attempt was made to involve the interested elderly people who stayed alone to do the job, but, due to difficulty in doing the procedure with the elderly, volunteers of the villages, who were intelligent and experienced enough to do the job, but, due to difficulty in doing the procedure with the elderly, volunteers of the villages, who were intelligent and experienced enough to do the job, were included in the study for pile sorting. A total of 16 such purposively chosen volunteers were included, who were intelligent and experienced enough to do the job, the investigator who carried out these exercises was trained in qualitative methods. One to two free listing or pile sorting activities were carried out in a single day. This study was conducted during July to December 2017.
Data analysis
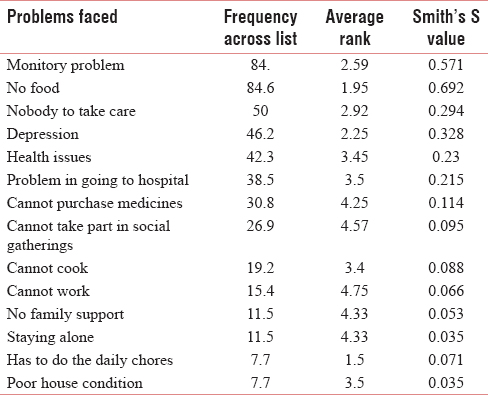
Smiths salience score was calculated and the reasons with higher Smith's S values were pile sorted. Smith's S value refers to the importance, representativeness, or prominence of items to individuals or to the group and is measured in following three ways: word frequency across the lists, word rank within the lists, and a combination of these two.[10] To get a collective picture, two-dimensional scaling and hierarchical cluster analysis of the pile sort data was done. To increase the validity of the results, the findings of free listing were pile sorted. The analysis of free list and pile sort data was done using Anthropac software.
RESULTS
How the life of “elderly staying alone” changed in due course of time?
The free exercise was carried out to identify the contents of domain, how life of “elderly staying alone” changed in due course of time. The contents have been enlisted in Table 1 in descending order of Smith's salience. The top five contents by importance, representativeness, or prominence are “feeling lonely,” “could not work,” “nobody to take care,” “feeling depressed,” and “nobody to talk/share feelings.”

Pile sort exercise [Figure 1] was carried out to unearth the structure of the domain – how life of “elderly staying alone” changed in due course of time and three main categories came up, namely, “no changes,” “changes at family level,” and “changes at societal level.” The subdomain “no change” has two contents: “could not elicit change” and “happy to be alone.” There was a small portion of the study population who did not elicit any change in their lifestyle since they were living alone. One of the respondent commented, “I am happy to be alone.”
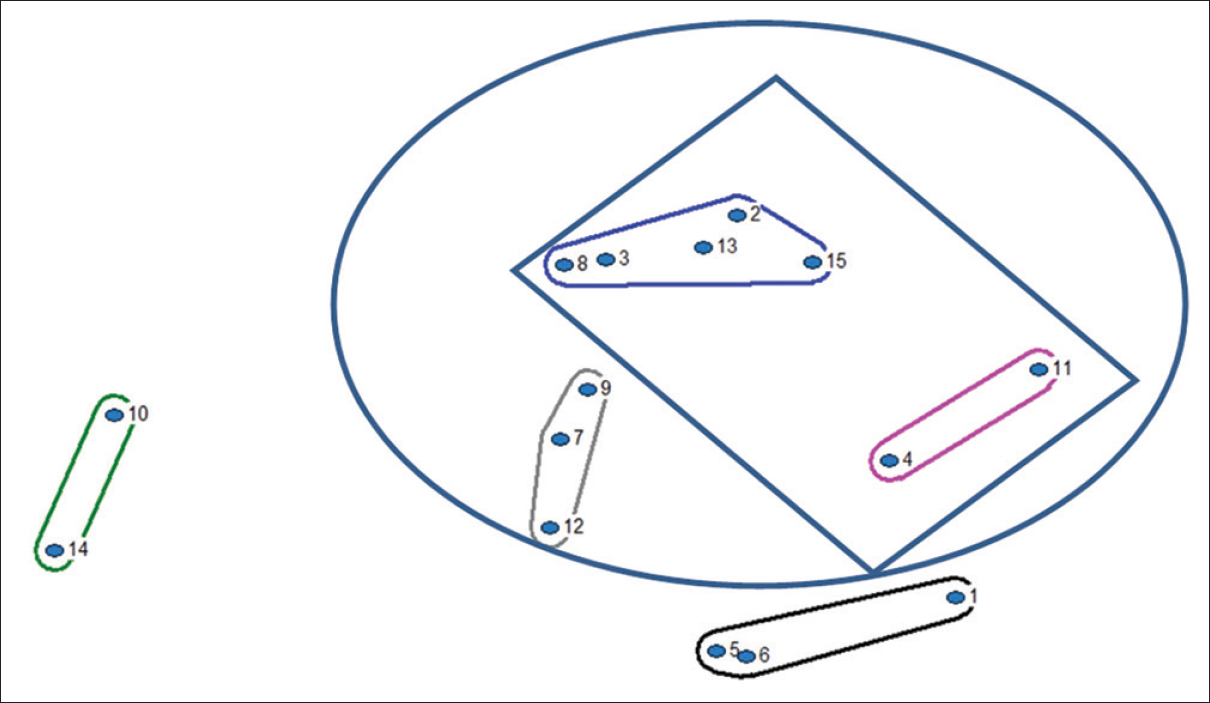
- How the life of “elderly staying alone” changed in due course of time
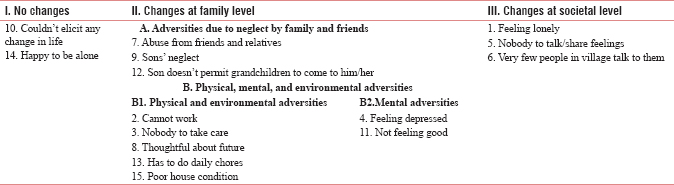
The second subdomain “changes at family level” has two parts, namely, “adversities due to neglect by family and friends” and “physical, mental and environmental adversities.” The subgroup “adversities due to neglect by families and friends” has three contents, namely, “ abuse from friends and relatives', 'sons' neglect', and 'son doesn't permit grandchildren to come to him/her.” The subgroup “physical, mental and environmental adversities” has five contents, namely, “cannot work,” “nobody to take care,” “thoughtful about future,” “has to do daily chores,” and “poor house condition,” and the subgroup “mental adversities” has two contents: “feeling depressed” and “not feeling good.”
The third subdomain “changes at societal level” has three contents: “feeling lonely,” “nobody to talk/share feelings,” and “very few people in village talk to them.”
During interviews, many of the study participants stated that they were being insulted from their siblings as well as other relatives. “My son does not allow me to talk and play with my grandson,” complained an elderly man. Many of them said that their sons neglected them and they receive abuses from others. Some of them are residing in houses, which are old and worn out, which has not been repaired since years. An elderly female participant of 70 years said, “my hut is by the side of the river and it may break anytime.” All these make them worried and thoughtful about their future.
What were the problems faced by them?
The contents of the second domain “problems faced by elderly staying alone” obtained by free listing are enlisted in Table 2 in descending order of Smith's salience value. The top five contents by importance, representativeness, or prominence for the second domain are monitory problems, no food, nobody to take care, depression, and health issues.
At the end of pile sort exercise, we got three major subdomains [Figure 2], namely, “poor social life,” “poor family support,” and “poor health care.” The first subdomain “poor social life” is made up of three contents, namely, “depression,” “cannot take part in social gatherings,” and “staying alone.” The second subdomain “poor family support” has two parts: “poverty” (made up of five components, namely, “monitory problems,” “no food,” “cannot cook,” “cannot work,” and “poor house conditions”) and “feeling of helplessness” (made up of three components, namely, “nobody to take care,” “no family support,” and “has to do daily chores”). The third subdomain “poor health care” has three contents: “health issues,” “problem in going to hospital,” and “cannot purchase medicine.”

- Problems faced by “elderly staying alone”
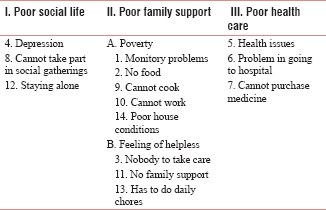
The discussion with the study participants cleared that the first and foremost major problem was poverty. Most important reason for their poverty was their inability to work like before due to their physical constraints. Due to lack of money, they could not arrange food or cook it. Monitory problems were also the reason for their poor condition of their houses. It is not only that the elderly people commonly found to suffer from different chronic illnesses such as diabetes, hypertension, backache, myalgia, poor vision, decreased hearing, or respiratory problems, but also an important problem was regarding visiting health facilities for their treatment or in purchasing medicines, due to lack of money and family support.
How did the elderly cope up with the various problems of being staying alone?
The free list exercise carried out for the third domain “ways of coping up with different problems faced by elderly staying alone” identified 17 different contents as per descending Smith's salience, which is enlisted in Table 3. The top five contents by importance, representativeness, or prominence are “begs or requests others for food,” “goes to government hospital,” “works in the field sometimes,” “utilizing old age scheme,” and “begs or requests others for money.”
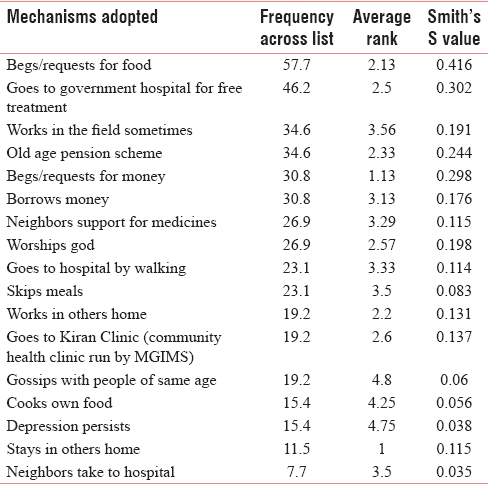
Pile sort exercise [Figure 3] for this domain came out with three major subdomains: “managing food and passing time,” “managing money,” and “meeting health needs.” The first subdomain “managing food and passing time” has six contents, namely, “begs/requests others for food,” “worships God,” “skips meals,” “gossips with people of same age,” “cooks own food,” and “stays in others home.” The second subdomain “managing money” includes the following six contents: “works in the field sometimes,” “old age scheme,” “begs/requests others for money,” “borrows money,” “works in others home,” and “depression persists.” The third subdomain “meeting health needs” contains the following five contents: “goes to government hospital,” “neighbors support for medicines,” “goes to hospital by walking,” “goes to village clinic,” and “neighbors take her/him to hospital.”
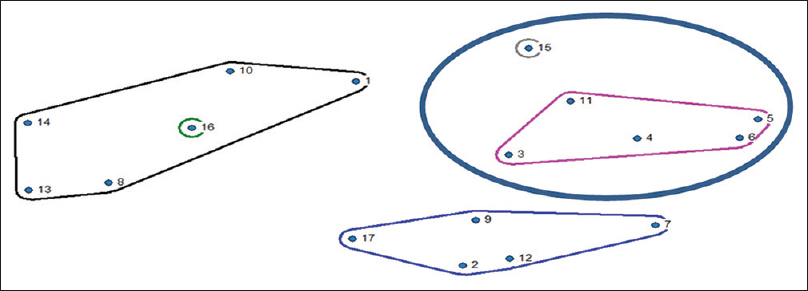
- Mechanisms adopted by elderly to cope up with various problems of being staying alone
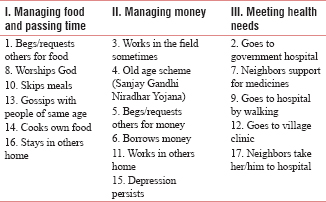
It has been found that many of them begs or requests their neighbors for food or sometimes skips meals and remain empty stomach. Some of them cook food themselves from the raw materials and vegetables that they purchase or get from the villagers. They pass their time by gossiping with other people, who were mostly of their age. Some of them said, worshipping God makes them feel happy and gives strength in surviving being alone. Some of them stay in others home, and this solves the problem of food as well as passing out time.
DISCUSSION
India, now home to 1.3 billion people, is projected to overtake China in about a decade to become the world's most populous country. Keeping the similar pace as that of the increasing Indian population, the share of India's elderly population aged 60 years and above is projected to rise from 8% in 2010 to 19% in 2050, as per the reports of United Nations Population Division (2011). This increase in the share of elderly will bring with it a variety of social, economic, and health-care policy challenges. In such a circumstance, the role of family is very vital.[11]
The family,[12] which is the primary unit of all societies is a group of biologically related individuals living together and eating from a common kitchen. India, though is famous for her culture of joint families, the recent statistics speaks against it. According to the 2001 census, in India, out of 19.31 crore households, 9.98 crore or 51.7% were nuclear households. In the 2011 census, the share grew to 52.1%–12.97 crore nuclear out of 24.88 crore households. The proprtion of joint families in India, meanwhile, fell substantially to from 19.1% (3.69 crore) to 16.1% (4 crore) across India. In rural areas, the dip was sharper – from 20.1% to 16.8% – than in urban India where it fell from 16.5% to 14.6%.[7] In this context of increasing trend of nuclear families, the worst sufferers are the elderly people. Their condition deteriorates when they lose their spouse and become all alone in the world.
The findings from this current study highlighted the different problems the “elderly staying alone” face. The most important reason which is the root cause of all problems is the lack of family support. It results in poverty, decreased health care and hygiene, hunger, poor housing conditions, which when coupled with neglect and abuse from the neighbors resulted in increased mental illnesses among the elderly population.
According to the Ministry of Social Justice and Empowerment, Government of India, in its document on the National Policy for Older Persons,[13] one-third of the elderly population is below the poverty line. The old age pension scheme comes under the domain of the concurrent list. Hence this pension schemes fall within the purview of both the central as well as state governments, which is an important measure in financially stabilizing the elderly population. Different states invest differently for elderly pension schemes. Some states contribute less while some more. In Maharashtra, the elderly population below poverty level receives a scheme called Sanjay Gandhi Niradhar Yojana, where they get 600 rupees per month benefit, but there are issues of timely distribution of the incentives as reported by our study participants. Many of them also said that this amount was too less and did not cater for all of their needs. There are no separate schemes for the “elderly people staying alone.” As they no more could work like before due to physical constraints, begging for food and money are reported to be the alternative ways to live their livelihood. But inspite of these endeavors, the money they get or could earn is very less as compared to their daily requirement to fulfill their basic needs that result in persistence of depression.
Remittances from children seem to be their main source of income of this age group of population.[14] However, the problem comes when there is nobody to take care or give remittances to the poor elderly people. Earlier, children traditionally used to take the responsibility of their old parents, but now, due to a number of reasons, they leave their parents and go away with their family, making the old people vulnerable to all the ill effects of being staying alone. According to the Maintenance and Welfare of Parents and Senior Citizens Act, 2007, under Section 24, if anybody who has responsibility for the care or protection of a senior citizen leaves him/her in any place, with the intention of wholly abandoning him/her, such person shall be punishable under the Act with imprisonment of either 3 months or fine up to rupees 5000 or both. The offense will be cognizable and will be tried by a Magistrate.
The National Policy on Older Persons of 1999 provides several welfare facilities for the elderly. It is found that a majority of elderly do not know of the existence of such policy and welfare schemes. Thus, it is essential to undertake urgent steps that could help in spreading awareness about the policy and welfare schemes at the ground level, so as to enable them to reap their benefits.[13] One of the shortcomings of the National Policy for Older persons is that it has not specified the actual total number of older persons below poverty line (BPL), which it intends to serve. Thus, it would be beneficial if a comprehensive survey is conducted to identify the total number of elderly persons belonging to BPL families.
Hence, inspite of all these measures taken by the government, the “elderly people staying alone” are still neglected, suffering from poverty and are socially deprived. There is no social structure that can take care of them. It is the high time for the government to step in for bringing societal and familial reforms that will safeguard this special elderly population of rural India.
There are few recommendations for developing the condition of the “elderly staying alone” in India, that may be at familial, societal, and policy level.
In the family level, the younger generation should be more thoughtful about the elderly in the homes and should not leave them all alone. In case they need to leave their villages for work, they should take the elderly people with them or should make alternative arrangements so that the eldest family member is not alone at home and does not become a victim of negligence and abuse. The elderly people enjoy the company of their grandchildren and the kids should not be prevented from mixing with their grandparents. They need regular health checkups and medications. It is the duty of the younger generation to cater for their needs in their last days and should not allow them to go into depression.
The societies need to be more elderly friendly, especially to those who are all alone in their last days of life. It should be realized that everyone has to pass through this stage 1 day or the other. Societies should have a dedicated place or a clubhouse for elderlies to meet, talk, gossip, and share their feelings. Some entertaining facilities can be arranged for them like playing indoor games such as carrom or cards. They may find it refreshing to have an evening stroll, so a park or dedicated pavement may be built in the surroundings for the elderly citizens.
The government should arrange for free health treatment, free food, free medicines, and clothes for the “elderly who stay alone” and it will be a step toward universal health coverage that India is trying to achieve sooner. Special pension allowance if started which will be dedicated only for the “elderly staying alone,” will give better financial independence to them. The nongovernment organizations may play an important role in rendering services dedicated to this special elderly group. The number of government-aided old age homes should be increased, even in rural areas, where they will have a place to stay, get food to eat, have regular health checkup, and a peer group with whom they can share their feelings. A separate administration should be established to work for the problems of the “elderly who are staying alone.”
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 2012. Aging in Asia: Findings from New and Emerging Data Initiatives Washington D C. Available from: https://www.ncbi.nlm.nih.gov/books/NBK92618/pdf/Bookshelf_http://esa.un.org/unpd/wppNBK92618.pdf
- United Nations, Department of Economic and Social Affairs PD. Volume 1 Comprehensive Tables (ST/ESA/SER.A/399) 2017. World Population Prospects - 2017 Revision. United Nations; Vol. 1:1-377. Available from: https://www.esa.un.org/unpd/wpp/Publications/Files/WPP2017_Volume.I_Comprehensive-Tables.pdf
- [Google Scholar]
- Living alone, loneliness, and psychological well-being of older persons in Singapore. Curr Gerontol Geriatr Res. 2011;2011:673181.
- [Google Scholar]
- Europe PMC funders group Europe PMC funders author manuscripts a framework for understanding old-age vulnerabilities. Ageing Soc. 2013;26:1-22.
- [Google Scholar]
- World Report on Ageing and Health. Luxembourg: World Health Organization; 2015.
- Office of the Registrar General and census Commissioner. Ministry of Home Affairs. Government of India. 2011. Office of the Registrar General and census Commissioner. Available from: http://censusindia.gov.in
- [Google Scholar]
- India's challenges to active ageing in the context of globalization and its solutions: A critical analysis. Int J Curr Res. 2017;9:60626-31.
- [Google Scholar]
- Old age homes in India : Sharing the burden of elderly care with the family. In: Irudaya Rajan S, Balagopal G, eds. Elderly Care in India. Vol 12. Singapore: Springer; 2017. p. :77-93.
- [Google Scholar]
- The preponderance of negative emotion words in the emotion lexicon: A cross-generational and cross-linguistic study. J Multiling Multicult Dev. 2004;25:266-84.
- [Google Scholar]
- United Nations. Department of Economics and Social Affairs, Population Division. 1950-2050. World Population ageing. Available from: http://www.un.org/esa/population/publications/worldageing19502050/
- [Google Scholar]
- Park's Textbook of Preventive and Social Medicine. Vol Vol. 24. Jabalpur, India: M/S Banarisdas Bhanot Publication; 2017. p. :391-4.
- Government of India. In: National Policy on Older Persons. New Delhi: Ministry of Social Justice and Empowerment; 1999.
- [Google Scholar]




