
Translate this page into:
Penile Metastasis Secondary to Bladder Cancer: A Report of Two Cases
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Penile metastasis secondary to primary bladder cancer is a rare entity and represents a challenging problem. The common mode of spread to the penis is by retrograde venous route. The overall outcome is dismal and most patients will die within 1 year even after optimum treatment. Here, we report two such cases.
Keywords
Carcinoma Urinary Bladder
Penile metastasis
Radiotherapy

INTRODUCTION
Penile metastasis is an extremely rare entity. Only very few cases have been reported till date in the literature.[1] The primary tumor most commonly arises from the genitourinary tract, especially bladder and prostate, with bladder being the most frequent primary location. Around 300 cases of carcinoma urinary bladder have been registered in last 5 years in our institution. We have found only two such cases of ca urinary bladder who developed penile metastasis. The most common symptoms are penile swelling, induration, ulceration, and sometimes also associated with priaprism. Secondary penile tumors are usually associated with disseminated disease and indicate a poor prognosis. The intent of treatment is usually palliative and treatment consists of local tumor excision, partial or total penectomy, radiation therapy.[2] Chemotherapy has also been tried to increase survival.
CASE REPORTS
Case 1
An 85-year-old male, smoker presented with painless gross hematuria for last 1 year. His routine blood investigations and chest X-ray were within normal limit. Contrast-enhanced computed tomography (CECT) scan showed polypoidal mass in the right posterolateral wall of urinary bladder with bilateral pelvic lymphadenopathy. His metastatic work up (including chest X-ray, CECT chest, abdomen and pelvis, and bone scan) was normal. Patient underwent transurethral resection of bladder tumor and postoperative histopathology revealed a high grade papillary urothelial carcinoma infiltrating the lamina propria and deep muscle. In view of old age and poor general condition of the patient, he was not taken up for radical cystectomy or concurrent chemoradiation. He was planned for radical radiotherapy alone 50 Gy in 25 fractions over 5 weeks with conventional four field technique in 6 MV linear accelerator. After nine fractions, of radiation patient complained of swelling and pain in his penis. Clinical examination revealed a 3 × 2 cm indurated swelling in the shaft of the penis. Magnetic resonance imaging (MRI) showed an ill-defined area of altered signal intensity appearing isointense to muscle on T1 and of intermediate signal intensity on T2-weighed images is seen involving bilateral corpora cavernosa with probable extension to the corpus spongiosum as well [Figure 1]. Fine needle aspiration cytology (FNAC) of the penile swelling revealed metastatic transitional cell carcinoma [Figure 2]. After nine fractions, radiotherapy plan was revised and radiation field was enlarged along with special wax bolus to accommodate the penile lesion. He completed radical radiation uneventfully and was kept on follow-up. No chemotherapy was offered because of old age and poor general condition of the patient. After 2 months of follow-up, he underwent MRI pelvis and both the bladder as well as penile lesion showed partial response. Patient is relieved from intractable pain and is leading a good quality of life.

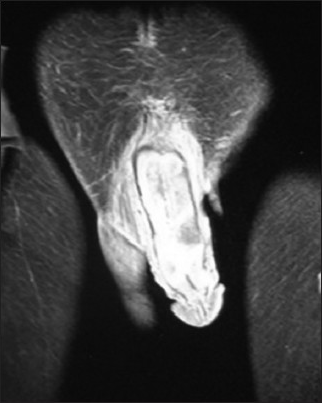
- MRI showed an ill defined area involving bilateral corpora cavernosa with probable extension to the corpus spongiosum as well
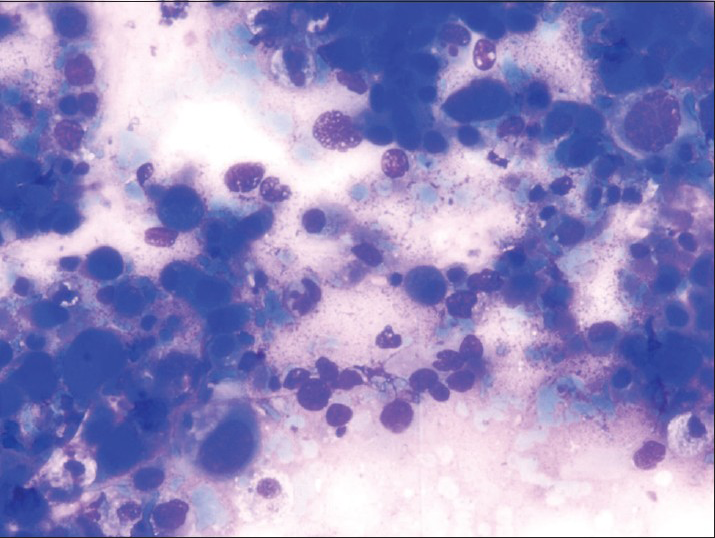
- Smear showing scattered round to oval malignant cells showing moderate nuclear pleomorphism (May Grünwald Giemsa stain)
Case 2
A 58-year-old male presented with hematuria for 1 month. He smoked one pack of cigarettes per day for last 30 years. He was thoroughly investigated and CECT scan revealed a soft tissue density mass in posterior wall of urinary bladder. He underwent transurethral resection of bladder tumor and histopathology showed high grade urothelial carcinoma with involvement of deep muscle. He received four cycles of neoadjuvant chemotherapy based on injection cisplatin 70 mg/m2 intravenous day 1 and injection gemcitabine 1.2 g/m2 day 1 and day 15. After four cycles of neoadjuvant chemotherapy, he underwent radical cystectomy with pelvic lymphadenectomy and ileal conduit diversion. Patient was kept on follow-up and after 4 months of surgery patient complained of painful swelling on glans penis. Clinical examination revealed indurated swelling at base of penis and another small nodule present at the shaft of the penis. MRI pelvis showed evidence of well-defined heterogeneous soft tissue mass of size 5 × 2.8 × 2 cm seen in left crura of the penis near its base. It was hyperintense on T2W1 and isointense on T1W1and it showed thick irregular peripheral enhancement [Figure 3]. Similar lobulated soft tissue lesion of size 1.8 × 1.9 × 1 cm was seen just medial to right puborectalis muscle. FNAC of penile lesion revealed metastatic carcinoma [Figure 4]. Positron emission tomography scan showed intensely fluorodeoxyglucose (FDG) avid Standardized uptake value (SUV) maximum 17.6) heterogeneously enhancing soft tissue mass seen in the proximal two-third of the shaft of the penis extending to left crura with intensely FDG avid well-defined nodules of variable sizes were noted in bilateral lung fields [Figures 5 and 6]. He received palliative external beam radiotherapy to pelvis 20 Gy in five fractions delivered over a period of 1 week and he was registered in our palliative clinic. He did not receive any further chemotherapy in view of poor general condition and was expired within 2 months.
- MRI showed evidence of well defined heterogenous soft tissue mass of size 5 × 2.8 × 2 cm seen in left crura of the penis near its base
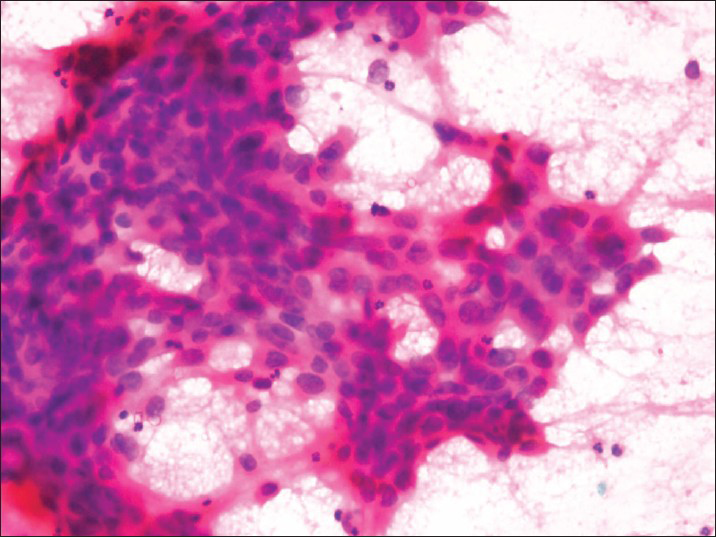
- Smear showing clusters of malignant cells showing moderate nuclear pleomorphism (H and E, stain ×40)
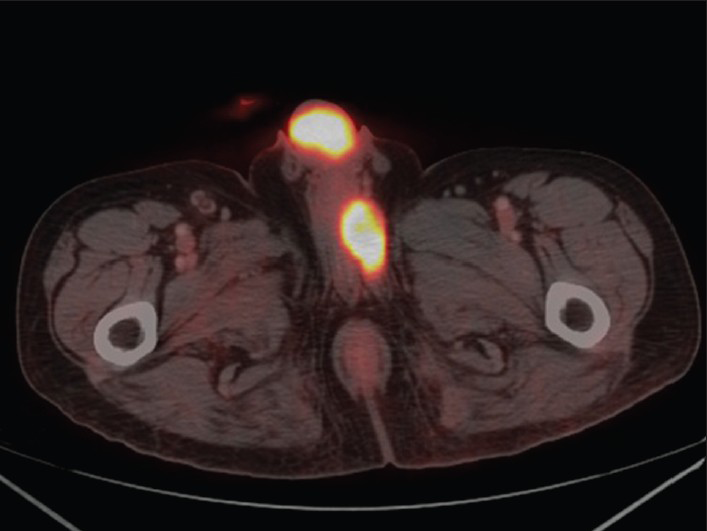
- PET scan showed intensely FDG avid (SUV maximum 17.6) heterogeneously enhancing soft tissue mass seen in the proximal two third of the shaft of the penis extending to left crura
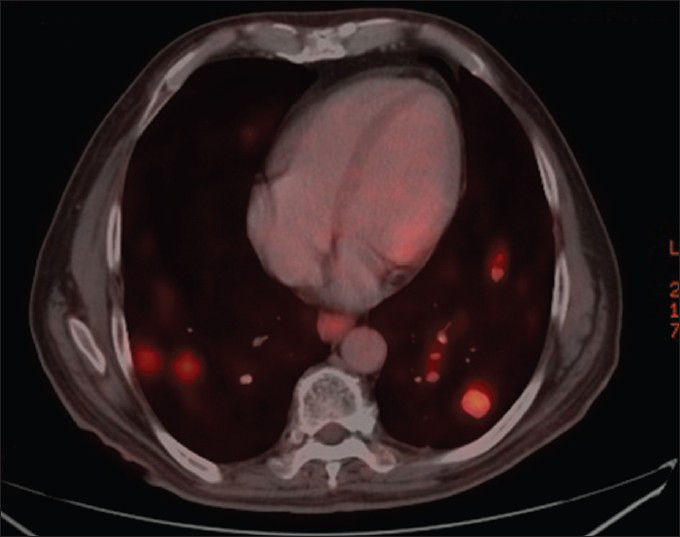
- Intensely FDG avid well defined nodules of variable sizes in bilateral lung fields
DISCUSSION
Metastasis to penis is a very uncommon presentation. Most commonly penile metastasis arises from urinary bladder and prostate, and less commonly from kidney, testes colon and rectosigmoid.[1] There are various mechanisms of penile metastasis reported in the literature. Metastatic spread from primary bladder cancer to penis occurs mainly via retrograde venous route. The other postulated mechanism for penile metastasis include retrograde lymphatic spread, direct invasion, direct arterial spread, and instrumental seeding.[3] Approximately, two thirds of all penile metastasis are detected at a mean time of 18 months after the detection of the primary tumor and reaming one third is presented at the same time with primary tumor.[4] In both the index cases, penile metastasis developed within 6 months of diagnosis. The main symptoms of penile metastasis are induration and swelling of penis.[5] Cherian et al.,[1] reported that up to 40% patients with penile metastasis may initially present with priapism, due to compromised penile venous drainage. Pain, hematuria, and obstructive voiding symptoms are rarer presentations.
The optimal treatment for penile metastasis requires a combined modality approach. Carcinoma bladder with penile metastasis is usually associated with dismal prognosis and the treatment is usually palliative. The average survival in patients with penile metastasis is 3.9 months from diagnosis and with extensive surgery and chemotherapy, a survival of 9.2 months has been reported.[6] The surgical treatment options are local tumor excision, partial or total penectomy. Other options for the management of a penile metastasis include external beam radiotherapy, brachytherapy, and chemotherapy.[1] Comparative trials do not exist due to rarity of this entity, but there have been isolated reports of disease remission with limited follow-up after undergoing nonsurgical management. The optimum treatment of this entity is not clear due to scarcity of data. More prospective studies are required to decide adequate treatment of this rare presentation. Our observation may throw some light in such cases.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Secondary carcinoma of the penis. A report of three new cases. Eur Urol. 1989;16:308-9.
- [Google Scholar]
- Secondary carcinoma of the penis; a review of the literature and report of nine new cases. Cancer. 1959;9:626-32.
- [Google Scholar]
- Penile metastasis from primary transitional cell carcinoma of the renal pelvis: First manifestation of systemic spread. BMC Cancer. 2004;4:90.
- [Google Scholar]
- Metastatic tumors to the penis: A report of 17 cases and review of the literature. Int J Surg Pathol. 2011;19:597-606.
- [Google Scholar]




